

To evaluate the current management of gout in general practitioners and specialists in Buenos Aires city.
Material and methodsMultiple choice, anonymous, survey, performed on 33 rheumatologists (REU), 52 Internal Medicine specialists (EMI) and 86 general practitioners (Otros).
ResultsGout is a very common or usual disease for 51.5% of REU vs 11.5% EMI and 8.1% Otros. At diagnosis, uric acid crystals are identified by 51.5% REU vs 28.8% EMI and 26.7% Otros and tophi observed by 60.6% REU vs 30.8% EMI and 30.2% Otros. REU and EMI should indicate colchicine for acute gout in 75.8% and 80.8% respectively vs 7.7% of Otros. REU measure patient's height/weight and waist circumference less frequently than EMI (66.7% vs 92.3% and 45.5% vs 75% respectively).
ConclusionsREU usually examine patients with gout but in a chronic stage. The identification of crystals in synovial fluid is low. The use of colchicine is still high. REU should improve the evaluation of the metabolic syndrome.
Evaluar la gestión actual de la gota en los médicos generales y especialistas en Buenos Aires.
Material y métodosPreguntas de selección múltiple, encuesta anónima, realizada a 33 reumatólogos (REU), 52 especialistas en medicina interna (EMI) y 86 médicos generales (Otros).
ResultadosLos REU atienden a pacientes con gota muy frecuentemente o habitualmente en un 51,5% de los casos vs. un 11,5% de EMI y un 8,1% de Otros. Al momento del diagnóstico, los cristales de ácido úrico fueron identificados por un 51,5% de REU vs. un 28,8% de EMI y Otros 26,7%; los tofos fueron identificados por un 60,6% de REU % vs. un 30,8% de EMI y un 30,2% Otros. Los REU y los EMI usan colchicina para la gota aguda en el 75,8 y el 80,8%, respectivamente, frente al 7,7% de Otros. La medida de altura/peso y la circunferencia de la cintura del paciente fue realizada con menos frecuencia por REU que por EMI (el 66,7 vs. el 92,3% y el 45,5 vs. el 75%, respectivamente).
ConclusionesLos REU suelen examinar a los pacientes con gota, pero en una etapa crónica. La identificación de los cristales en el líquido sinovial es baja. El uso de colchicina sigue siendo alto. Los REU deben mejorar la evaluación del síndrome metabólico.
Although gout has been described since antiquity and its treatment includes drugs used for millenia,1 it remains an under-diagnosed disease or is diagnosed at later stages and, even when correctly diagnosed, treatment is usually suboptimal.2 Unlike rheumatoid arthritis or systemic lupus erythematosus, gout seems to be regarded by rheumatologists as a minor illness and its diagnosis and management usually falls to general practitioners.3
The aim of this study was to assess the current management of gout by general practitioners and specialists in the city of Buenos Aires and its surrounding areas.
Materials and MethodsAn anonymous, closed, multiple-choice survey was applied to doctors from the city of Buenos Aires and surrounding areas, between May 2010 and May 2011.
The initial development of the survey was conducted by 2 authors (NF and GS) on the basis of: (a) changes made to a survey used in a previously published study by other authors4 (JVM) and (b) other publications.2,5,6
The survey was modified and finally accepted by the consensus of all authors: the survey tried to find out what professionals do in their daily practice. It consisted of 18 questions and included a first part with professional data, frequency of patients evaluated for gout (too often, usually infrequently and rarely) and number of patients seen per month (between 1 and 5, between 6 and 10, between 11 and 20, over 20).
In the second part, we asked about the manner in which gout patients are commonly attended and how the diagnosis of gout was made, with special emphasis on the detection and identification of monosodium urate crystals (MUC) in synovial fluid or tophi. The third part assessed the treatment of acute and chronic gout. We also evaluated the indications for lifestyle modifications and changes and, finally, asked about 5 measures for evaluation of the metabolic syndrome.
Rheumatologists (REU), internal medicine specialists (EMI) and physicians without specialty, or other physicians who worked mostly in emergency services (Other) were surveyed.
Surveys were completed personally by professionals assisting to different scientific events related to rheumatology, held in the City of Buenos Aires in that period. We also visited several emergency rooms and medical clinics in Buenos Aires, where other professionals completed the survey.
While there was strict control of the percentage of professionals contacted who agreed to answer the survey, it is estimated that the percentage of participation did not exceed 20% of professionals who were contacted personally. We also sent 75 emails, with a copy of the survey from a closed contact at the Rheumatology department of the Hospital JM Ramos Mejia, and 19 professionals answered (6 REU, 6 and 7 Others EMI).
For the analysis we used descriptive statistics and χ2 test (significant P<.05) and SPSS for Windows version 17.0 software.
ResultsOne hundred seventy-one physicians responded to the questionnaire: REU 19.3%, EMI 30.4% and 50.3% Other. The other group had fewer years of professional experience: only 18.6% of the Other group had more than 10 years vs 36.4% of the REU and 38.5% of the EMI (P<.021).
Patients most commonly assessed by REU and EMI were those with hyperuricemia with or without a diagnosis of gout (48.5 and 46.2%, respectively), while for the other 39.5%, acute monoarthritis was the most frequent form of presentation.
REU cared for gout patients very frequently or habitually in 51.5% of cases vs EMI 11.5% and 8.1% Other (P<.001). The REU examined between 1 and 5 gout patients per month in 81.82% of cases, EMI in 96.15% and Others in 96.51%, while 18.18% of the REU, 85% of EMI and 3.49% of Others saw more than 5 patients with gout per month (P=.009).
Physicians were asked if they based their diagnosis on clinical gout, hyperuricemia, the presence of tophi, identifying MUC or a combination of the above.
To diagnose gout, clinical data (alone or combined with other criteria), were used by 93.9% of the REU, 92.3% of EMI vs 72.1% Other (P<.01). The study and identification of MUC were used for diagnosis (alone or combined) by 51.5% of REU vs 28.8% of EMI and 26.7% Others (P=.010). The presence of tophi (alone or combined) was reported by 60.6% of REU vs 30.8% EMI and 30.2% of Others (P=.005). Hyperuricemia was used by 42.4% of REU, 44.2% of EMI and 43% Others (P=.98, NS).
In the ideal case of a patient with acute monoarthritis and a history of gout, 75.8% of REU would perform articular puncture vs 44.2% of EMI and 30.2% Others (P<.001).
Over 80% of respondents would use nonsteroidal antiinflammatory drugs (NSAIDs) alone or in combination for acute gout.
REU and EMI indicate colchicine more alone or combined frequently: 75.8% and 80.8%, respectively, vs 47.7% Other (P<.001). 32.6% of the Others included allopurinol in the treatment of acute gout vs 19.2% of the EMI and 6.1% of the REU (P=.007).
With respect to the use of allopurinol, we found that REU used it later (after the second attack) in 60.6% vs 15.4% of EMI and Others 14% (P<.001). 84% of the REU recognized that concomitant treatment for the prevention of acute gout (NSAID or colchicine) is indicated when starting treatment with allopurinol vs 46.2% of EMI and 37.2% Others (P<.001).
Ideally, in cases of renal failure, liver and tolerability of the drug, 42.4% of REU, 44.2% EMI and 44.2% Other (P=.98, NS) would use higher doses of 300mg of allopurinol/day.
The goal of treatment with allopurinol is to lower uric acid to less than 6mg/dl according to 72.7% of REU, 57.7% of EMI and 48% of Others (P=.06, NS).
Allopurinol was maintained indefinitely by 90.9% of REU vs 61.5% of EMI and 57.0% of Others (P=.002).
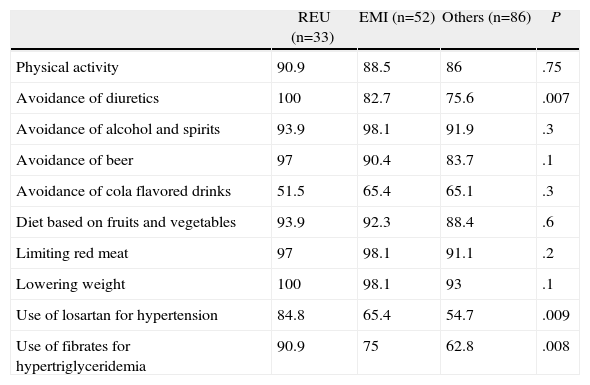
On a list of 10 preventive measures, doctors’ responses differed only in (Table 1):
- 1
Avoid the use of diuretics: 100%. Of REU vs 82.7% EMI and 75.6% Other (P=.007).
- 2
Suggest the use of losartan in cases of hypertension by 84.8% REU vs 65.4% of EMI and Others 54.7% (P=.009).
- 3
Suggest the use of fibrates in case of hypertriglyceridemia: 90.9% of REU vs 75.0% of EMI and 62.8% Others (P=.008).
Frequency With Which Those Surveyed Indicated 10 Diet and Lifestyle Recommendations (%).
| REU (n=33) | EMI (n=52) | Others (n=86) | P | |
| Physical activity | 90.9 | 88.5 | 86 | .75 |
| Avoidance of diuretics | 100 | 82.7 | 75.6 | .007 |
| Avoidance of alcohol and spirits | 93.9 | 98.1 | 91.9 | .3 |
| Avoidance of beer | 97 | 90.4 | 83.7 | .1 |
| Avoidance of cola flavored drinks | 51.5 | 65.4 | 65.1 | .3 |
| Diet based on fruits and vegetables | 93.9 | 92.3 | 88.4 | .6 |
| Limiting red meat | 97 | 98.1 | 91.1 | .2 |
| Lowering weight | 100 | 98.1 | 93 | .1 |
| Use of losartan for hypertension | 84.8 | 65.4 | 54.7 | .009 |
| Use of fibrates for hypertriglyceridemia | 90.9 | 75 | 62.8 | .008 |
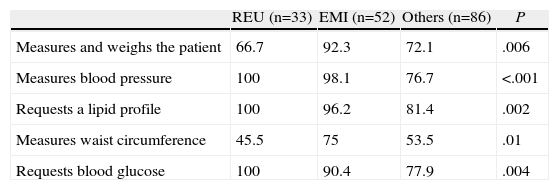
Regarding the five measures for the evaluation of the metabolic syndrome (Table 2), REU measure blood pressure, blood glucose and lipid profile in the same proportion as the EMI, but they measured height/weigh of the patient only sometimes: 66.7% vs 92.3% of EMI (P=.006). REU also measure waist circumference less often than EMI (45.5% vs 75%, P=.01).
Frequency of Evaluation of Parameters of Metabolic Syndrome by Those Surveyed (%).
| REU (n=33) | EMI (n=52) | Others (n=86) | P | |
| Measures and weighs the patient | 66.7 | 92.3 | 72.1 | .006 |
| Measures blood pressure | 100 | 98.1 | 76.7 | <.001 |
| Requests a lipid profile | 100 | 96.2 | 81.4 | .002 |
| Measures waist circumference | 45.5 | 75 | 53.5 | .01 |
| Requests blood glucose | 100 | 90.4 | 77.9 | .004 |
Professionals were asked whether they referred the patient to the REU and the answers were: (a) never: 3.85% of EMI and 9.30% Others; (b) after the first attack: 46% and 40.70% of EMI and Others, respectively; (c) after the second attack: 15.38 and 22.09% of EMI and Others, respectively; (d) patients with polyarticular disease with tophi or no response to treatment: 42.31% and 27.91% of the EMI and Other, respectively.
DiscussionAlthough there are guidelines for the diagnosis and treatment of gout, there is evidence that patients with gout are not treated correctly.7,8 From our data it appears that about 40% of EMI and other physicians never refer patients to the rheumatologist or only do so in the presence of a case of polyarticular tophi, complications or treatment failure. Thus, rheumatologists see patients late in the clinical course of the disease, since referring doctors rely on the presence of tophi for diagnosis in 60% of cases. The search and identification of MUC and articular puncture (necessary to confirm the diagnosis) are used in a significantly higher manner by REU, who are probably better-trained in these techniques.
Colchicine is still an option for the treatment of acute gout for a major portion of REU and EMI.
REU tend to maintain allopurinol longer and use it more frequently with concomitant medication at the onset of therapy.
Rheumatologists surveyed considered metabolic syndrome and evaluated it in a similar way than clinicians, but should weigh patients and take other measurements more frequently.
Different surveys were published in the last 10 years on the diagnosis and treatment of gout.4,5,9–11 The participation of professionals in these surveys, overall, was low.
While in some surveys5,9 more than 80% of rheumatologists reported finding and identifying MUC, our results were similar to those reported in Mexico in 2003, where 51% of rheumatologists and 30% of internists used this as a diagnostic4 method.
In this survey, the use of colchicine by the REU was higher than reported in the U.S. in 2006.5
It is possible that physicians in the polls express their opinions or their academic knowledge and not necessarily what they really do in clinical practice, which is evident when performing audit work on patient files.12
Among the strengths of our study we can note that, in addition to REU, we included general practitioners (who worked mostly in emergency rooms) and EMI.
Hyperuricemia and gout are closely linked to the metabolic syndrome13,14 or cardiovascular15 risk. This entails taking a broader view of gout, where joint involvement is only part of the problem. This survey included a section on the evaluation and management of metabolic syndrome.
Under the constraints of a survey and the low turnout, this data cannot be directly extrapolated to all doctors in Buenos Aires.
However, the data is disappointing and, in the absence of similar studies, it is a starting point to estimate adherence to treatment guidelines and quality of care received by patients with gout in the Autonomous City of Buenos Aires.
In conclusion, patients with gout should be referred earlier to REU in order to confirm the diagnosis and improve care.
Ethical disclosuresProtection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of Data. The authors declare that no patient data appears in this article.
Right to privacy and informed consent. The authors declare that no patient data appears in this article.
Conflict of InterestThe authors declare no conflict of interest.
Please cite this article as: Fara N, et al. Una encuesta sobre la evaluación y el tratamiento actual de la gota en Buenos Aires, Argentina. Reumatol Clin. 2012;8:306–9.
This work was presented as a poster at the 44.° Congreso Argentino de Reumatología, held from 12 to 15 October 2011 in the city of Rosario, Argentina.
- Spontaneous pneumomediastinum: An extra muscular manifestation of anti-MDA5 dermatomyositis. Report of 2 cases
- The impact of COVID-19 and other factors on the usage status of the biologic drug therapies for rheumatoid arthritis: A study from Vietnam
- Analysis of factors involved in the development of humoral response to vaccination against SARS-CoV-2 in patients with rheumatic pathology under biological treatment
- The “autoimmune/inflammatory syndrome induced by adjuvants” (ASIA) after COVID-19 infection: A case report


