

Interstitial lung disease (ILD) as part of systemic sclerosis (SS) is a leading cause of morbidity and mortality.
ObjectivesTo evaluate the use of intravenous pulse cyclophosphamide combined with low and high doses of prednisone in the treatment of ILD in SS is equally effective.
MethodAn experimental, exploratory and randomized single-blind clinical trial was conducted at Hermanos Ameijeiras Clinical Surgical Hospital from September 2006 to December 2009, including 23 patients with SS and ILD. Two treatment schedules were evaluated and randomly assigned. Group A was composed of 13 patients with a monthly dose of cyclophosphamide (ev) for 6 months and a twice-monthly dose for the remaining 6 months, prednisone (1mg×kg×day) 4 weeks and then the dose was lowered to 5mg every 2 weeks up to 10mg. Group B: 10 patients with cyclophosphamide (ev), oral prednisone 10mg daily.
ResultsThere are significant differences at onset of CVF and the honeycomb pattern between both groups, where the high dose group was at a disadvantage. At the end of treatment the low dose group achieved improvement of radiologic lesions and the Warrick index, unlike the high dose group. The remaining variables experienced improvement in both groups without marked inequality. Similarly, slight adverse reactions were present in both groups. Two patients dropped out of the study.
ConclusionsA combination of low dose steroids with cyclophosphamide is effective in interstitial lung disease treatment especially in active disease, and results did not show differences regarding the high dose group but the sample size and the evolutionary severity of high dose patients oblige other studies to verify these data.
La neumopatía intersticial (NI) en el curso de la esclerosis sistémica (ES) constituye la causa principal de morbilidad y mortalidad.
ObjetivosEvaluar si el uso de prednisona en altas o bajas dosis combinado con ciclofosfamida intravenosa (iv) resulta igualmente eficaz en el tratamiento de la NI en la ES.
MétodoSe realizó un estudio explicativo experimental tipo ensayo clínico, aleatorizado y a simple ciego, donde se reclutó a 23 pacientes con ES y NI. Se evaluaron dos esquemas de tratamientos; grupo A: 13 pacientes con ciclofosfamida (iv) mensual durante 6 meses y bimensual durante los 6 meses restantes, prednisona (1mg×kg×día) 4 semanas y después se rebajó la dosis a 5mg cada 2 semanas hasta 10mg, y grupo B: 10 pacientes con ciclofosfamida (iv) y prednisona por vía oral 10mg diaria.
ResultadosSe muestran las diferencias significativas al inicio del estudio en la CVF y el patrón en panal de abejas entre ambos grupos, resultando desfavorecido el grupo de dosis altas. Al concluir el tratamiento, el grupo de bajas dosis logró una mejoría de las lesiones radiológicas y del índice de Warrick, a diferencia del grupo de dosis altas. Las restantes variables experimentaron mejoría en los dos grupos, sin marcada desigualdad. Se presentaron de forma similar reacciones adversas ligeras. Dos pacientes abandonaron la investigación.
ConclusionesUna combinación de dosis bajas de esteroides con ciclofosfamida es eficaz en el tratamiento NI especialmente en las formas activas. Los resultados no muestran diferencias respecto al grupo con altas dosis, pero el tamaño muestral y la mayor gravedad evolutiva de los pacientes con altas dosis, obligan a otros estudios para confirmar estos datos.
Systemic sclerosis (SS) is a multisystem disease of unknown etiology, characterized by inflammatory, vascular and fibrotic changes primarily affecting the skin and other internal organs, especially lungs, kidneys, heart and gastrointestinal1 apparatus. Approximately 40% of patients develop moderate to severe restrictive lung disease, where the biggest decline in lung function occurs in the first 3–5 years since the onset of symptoms.2 Interstitial lung disease (ILD) is the leading cause of morbidity and mortality in this disease and has a very variable course, so the subgroup of patients who will develop into a rapid pulmonary3 aggressive disease has not been identified.
Once interstitial fibrosis occurs, it is resistant to current treatment modalities, so it is very likely that aggressive therapy with immunosuppressive agents may be very effective at the beginning of the process.4 The development of diagnostic methods such as computed tomography (CT) and bronchoalveolar lavage cytology allows for the identification of ILD in its first stages.5
Several agents have been evaluated as treatment, but only oral or intravenous cyclophosphamide has proven effective. The results indicate that cyclophosphamide has modifying effects on lung function and response measures, such as dyspnea, quality of life, functional capacity and thickness of the skin.6,7 There is little evidence from studies evaluating the association between steroids and cyclophosphamide in the treatment of ILD. Pakas et al.8 and Wanchu et al.9 report improvement in respiratory function with cyclophosphamide and high doses of prednisone, so we decided to evaluate whether the use of prednisone in high or low doses combined with intravenous cyclophosphamide is equally effective in the treatment of ILD in SS.
MethodsWe performed an exploratory, experimental and clinical study, randomized, single blind at the Ameijeiras Brothers Hospital during the period from September 2006 until December 2009. The study included 23 patients with ILD that met the criteria for classification of SS (ACR 1980)10 and excluded patients with obstructive lung disease with VEF1/capacity FVC (FVC)>70% than predicted, a history of occupational exposure and patients with disorders that affect lung function as IMA, congestive heart failure, severe valvular disease, emphysema and pulmonary hypertension.
ILD was considered in patients with SS, the presence of a pattern of pulmonary ground glass or honeycombing on high resolution CT and/or the presence of active alveolitis in bronchoalveolar lavage fluid cell count with clinical dyspnea on exertion, accompanied by a decrease in FVC in the lung function test (LFT).11 This research protocol was approved by the scientific committee of the Hermanos Ameijeiras Hospital center of the Ministry of Health of the Republic of Cuba, and participants gave written agreement. Patients were randomized to two treatments. Each patient was enrolled consecutively, after assessing the above criteria, and was included in the study and was assigned to the corresponding treatment, with the help of a list of random numbers previously obtained by a computer using Asal. Two groups of patients were formed with different treatment regimens:
- –
Group A, high doses (13 patients) were administered intravenous cyclophosphamide at a rate of 0.75mg to 1g×m2 body surface area (maximum dose 1g) monthly for 6 months and bimonthly the 6 remaining months, plus prednisone at 1mg×kg daily for 4 weeks and then decreasing the dose at 5mg every 2 weeks until 10mg.
- –
Group B, low doses (10 patients) were administered the same cyclophosphamide dose and similarly to the first group, received combined oral prednisone 10mg daily. For prevention of nausea and vomiting, ondansetron was administered (8mg) plus intake of 3–4l of water to prevent hemorrhagic cystitis.
Complete clinical examination was performed, including measurement of the dyspnea index and the index of skin thickness (modified Rodnan). Patients were classified as diffuse and limited clinical skin forms using the LeRoy12 extension.
Investigations: complete blood count, platelets, ESR, creatinine, glucose, AST, ALT, CPK, LDH, Addis 2h, 24h proteinuria, serology (VDRL), HIV, hepatitis C virus antibody, surface antigen, antinuclear antibodies (ANA×IF), echocardiogram, chest radiograph, RFT, CT, bronchoscopy and bronchoalveolar lavage cytology.
Blood count was performed 15 days after each pulse of cyclophosphamide, with dose adjustments when the leukocyte count <3×109.
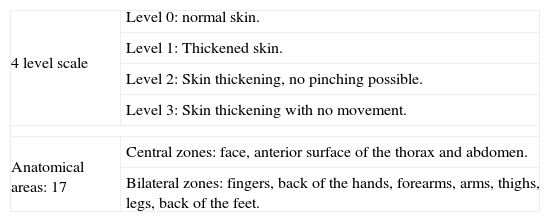
Dyspnea was assessed using a Likert scale (Table 1) 0–4 points grading from low to high degree of dyspnea: 0: none, 1: dyspnea on exertion after two flights of stairs, 2 dyspnea on exertion after a flight of stairs, 3 for dyspnea less than one flight of stairs or on the plain at their own pace, 4: dyspnea at rest.
Skin Thickness Index (Modified Rodnan).13
| 4 level scale | Level 0: normal skin. |
| Level 1: Thickened skin. | |
| Level 2: Skin thickening, no pinching possible. | |
| Level 3: Skin thickening with no movement. | |
| Anatomical areas: 17 | Central zones: face, anterior surface of the thorax and abdomen. |
| Bilateral zones: fingers, back of the hands, forearms, arms, thighs, legs, back of the feet. | |
Maximum score: 51 units.
RFT was performed using an ERGOCID-plus computer. By performing spirometry, inspiratory and expiratory forced inspiratory volume were measured.14 A restrictive pattern was defined when there was a fall in FVC≤80%.
Intensity: considered mild (79%–65%), moderate (64%–49%). severe (48%–35%) and severe (<34%).
Lung CTs was performed on a multislice CT scanner with 40 channels for multiplanal reconstruction, with 0.1mm slices. This study revealed the presence of two patterns, abnormal and the normal pattern. ILD was demonstrated by the presence of two patterns of abnormal appearance (“ground glass” and “honeycomb”).15
The “ground glass” appearance was defined by an increased density of the lung parenchyma, a fine reticular pattern of curvilinear opacities which are radio transparent spaces between 1 and 2mm in diameter. The presence of ground-glass opacities in the posterior basal subpleural courts was searched for in the prone position to exclude the possibility of gravitational effects that cause increased parenchymal density. The second pattern that looks like a honeycomb lattice medium was defined as subpleural lines, thickened septal or subpleural parenchymal borders and air space having a diameter between 3 and 10mm.
Readings and semiquantitative assessment of pulmonary radiological deterioration were made using the Warrick16 index and performed by two radiologists; any difference in interpretation was resolved by consensus. Elemental lesions were considered when the scores from one to 5 according to the severity were 1, ground glass opacities; 2, pleural irregularities in the edges; 3, lines by septal thickening and subpleural interlobular septa (1 thickening linear cm of the pleura), 4, honeycomb, and 5, subpleural cystic areas of wall thickening.
Also, Warrick's score assigns values between 1 and 3 according to the number of segments affected by the type of injury. A score of 1 indicates that the lesion is present in 1–3 segments; a score of 2 is present in 4–9 segments, and score 3 lesions are present in more than 9 segments. The scores for severity and extent of injury were added to provide a total CT score ranging from 0 to 30.
Bronchoscopy and washing cytology: the percentage of polymorphonuclear leukocytes≥3% and the percentage of eosinophils≥2% were considered pathological; therefore those were considered as an active17 bronchoalveolar lavage.
Clinical evaluation was performed and a blood count with differential was performed each month before administering cyclophosphamide.
Final assessment: at the end of treatment we performed a thorough clinical examination, including measurement of the levels of dyspnea and skin thickness, hematological tests, echocardiogram, chest radiograph, RFT, CT, bronchoscopy and cytological lavage. Two patients were not evaluated after they dropped out.
Statistical Data AnalysisThe collected data were processed using SPSS Vs11.5. Descriptive statistics were used for qualitative variables (absolute and relative frequencies) and for quantitative variables (mean±or standard deviation). To determine the homogeneous distribution of the two groups in baseline conditions, we used a homogeneity test statistic such as the chi-square, and the use of nonparametric Mann–Whitney test was used to calculate the average difference between the two groups for the duration of the disease. We also used the Wilcoxon test for related samples to evaluate the change in lung expansion obtained after treatment by Warrick index.
We considered a group of key variables after treatment analyzed in each group and compared to each other using the nonparametric Mann–Whitney tests.
In all statistical tests employed we considered a significance level of 0.05.
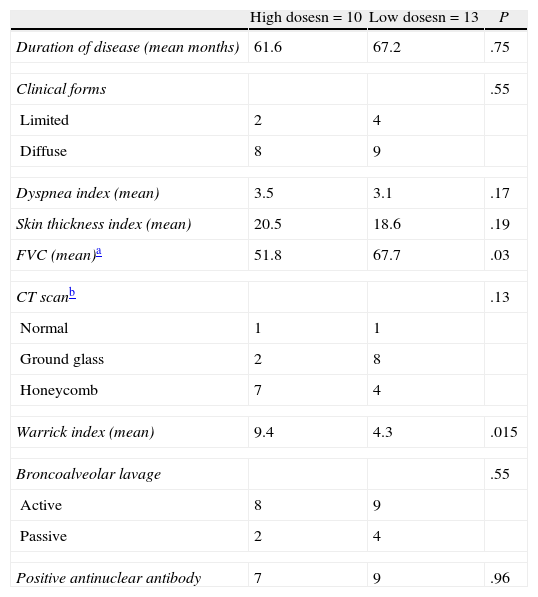
ResultsIn Table 2, shows the baseline characteristics of both groups: group A was composed of 10 patients, all women, with a duration of disease of 61.6 months, 8 with a diffuse clinical form and 2 limited. We obtained a 3.5-dyspnea index and skin thickness of 20.5; there was a predominance of active bronchoalveolar lavages. This group had a lower mean value of FVC, more patients with a honeycomb pattern and a higher Warrick score compared with group B. Total patients with positive ANA were 7. In group B, 13 patients, all women, and a time of disease progression of 67.2 months, 9 were of the diffuse clinical form and 4 of the limited, with a predominantly ground glass pattern on CT and active bronchoalveolar lavage, and a rate of dyspnea and a skin thickness of 3.1 and 16.8, respectively, with ANA-positive in 9 patients. One patient in each group did not complete the study. In group A one patient died due to pulmonary thromboembolism after completing one month of treatment, and in group B one patient was discontinued because she developed hemolytic anemia after the third month of treatment. None of the causes of abandonment was attributed to treatment.
General Initial Characteristics.
| High dosesn=10 | Low dosesn=13 | P | |
| Duration of disease (mean months) | 61.6 | 67.2 | .75 |
| Clinical forms | .55 | ||
| Limited | 2 | 4 | |
| Diffuse | 8 | 9 | |
| Dyspnea index (mean) | 3.5 | 3.1 | .17 |
| Skin thickness index (mean) | 20.5 | 18.6 | .19 |
| FVC (mean)a | 51.8 | 67.7 | .03 |
| CT scanb | .13 | ||
| Normal | 1 | 1 | |
| Ground glass | 2 | 8 | |
| Honeycomb | 7 | 4 | |
| Warrick index (mean) | 9.4 | 4.3 | .015 |
| Broncoalveolar lavage | .55 | ||
| Active | 8 | 9 | |
| Passive | 2 | 4 | |
| Positive antinuclear antibody | 7 | 9 | .96 |
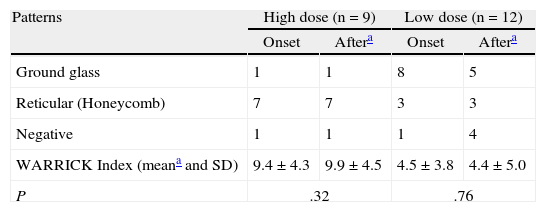
In the low dose group we evidenced an improvement in the radiological lesions and the Warrick index, with the high dose group differing, with a slight worsening of Warrick performance and no changes in radiological lesions (Table 3).
Behavior of the Patterns of Lung Affection and the Warrick Tomographic Index.
| Patterns | High dose (n=9) | Low dose (n=12) | ||
| Onset | Aftera | Onset | Aftera | |
| Ground glass | 1 | 1 | 8 | 5 |
| Reticular (Honeycomb) | 7 | 7 | 3 | 3 |
| Negative | 1 | 1 | 1 | 4 |
| WARRICK Index (meana and SD) | 9.4±4.3 | 9.9±4.5 | 4.5±3.8 | 4.4±5.0 |
| P | .32 | .76 | ||
One patient in group A (ground glass pattern) and a patient in group B (honeycomb pattern) did not finish the study.
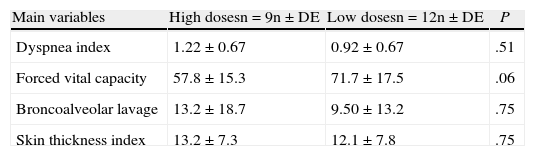
The clinical variables, the dyspnea index and improvement in skin thickness changes were seen in both groups, just as bronchoalveolar lavage and forced vital capacity. None of them showed significant differences between groups (Table 4).
Main Variables Measured After Treatment.
| Main variables | High dosesn=9n±DE | Low dosesn=12n±DE | P |
| Dyspnea index | 1.22±0.67 | 0.92±0.67 | .51 |
| Forced vital capacity | 57.8±15.3 | 71.7±17.5 | .06 |
| Broncoalveolar lavage | 13.2±18.7 | 9.50±13.2 | .75 |
| Skin thickness index | 13.2±7.3 | 12.1±7.8 | .75 |
Mann–Whitney's non-parametric test was employed.
Both groups had similar minor adverse reactions (nausea and vomiting) that were resolved with the administration of antiemetics.
DiscussionWe determined the effectiveness of high or low dose of cyclophosphamide associated with prednisone in the treatment of ILD in the course of SS. A search of the literature provides very few studies specifically performed to review this association. There are many papers which evaluate the efficacy of cyclophosphamide and, to a lesser extent, the use of cyclophosphamide and steroids, rarely comparing the efficacy of cyclophosphamide with high or low dose of prednisone, as performed by Pakas et al.8 Of the 23 patients with ILD, 73% are of the diffuse clinical form and 27% were limited. The presence of ILD is reported in up to 90% of the diffuse form and associated with the presence of SCL-7018 antibodies. The limited form usually has an indolent course with a predominance of vascular involvement, but in patients with prolonged illness and dyspnea can lead to lung disease,19 which is evident in the group of low-dose prednisone. Of the 13 patients included, there are only 4 with the limited clinical form, but have dyspnea as the main symptom and a longer history of disease.
ANA positivity was around 70%, a value lower than that reported in other regions, reflecting its presence in 90%–95%.20 We think that the method used (immunofluorescence and rat liver substrate) may be related to these results, although a recent study in our geographic area, Puerto Rico, displays ANA positivity in 66.7% of patients.21 A limitation of the study is absence of specific autoantibodies related to lung disease.
CT patterns in group A showed no regression and motivated primarily because this group included more patients with a honeycomb pattern corresponding to established lung fibrosis, where the response to treatment is lower. With these elements, group A shows a greater severity, yet, when we tried to strike a balance between groups by random assignment of patients, it was seen as weak and foreign to our purpose. In contrast, in group B there was regression of lesions in 50% which does not correspond to what has been achieved by Pakas et al. in those who were in the group of high dose steroids. The course of systemic sclerosis is characterized by parenchymal lung injury followed by inflammation and subsequent fibrosis.22 The initial inflammation corresponds to a ground glass pattern on CT and active alveolitis on bronchoalveolar lavage identifying an inflammatory stage is this the right time to start immunosuppressive23 therapy. In the high dose patients there was a higher percentage of mean reticular involvement that corresponds to the fibrosis seen on histological examination, which is considered the reason for the worsening of the Warrick index. Patients with this impairment have a greater restriction of lung function, however, both groups showed improvement in FVC in the same range. Although not directly related to the study variables and FVC Warrick index, it was found that patients in group A have a higher average value in the Warrick index and small FVC relative to group B. This inverse relationship is due to the predominance of honeycomb pattern in group A, which increases the index score (by greater severity and extent of lung injury), with the consequent decrease in the mean value of FVC and development of restrictive lung disease. In group B, a lower index value associated with the presence of a ground glass pattern, mainly on the lung bases and periphery, provides a lower score for the severity and extent of injuries, and expresses a lower impairment of FVC. A restrictive pattern is associated with severe dyspnea, anti-SCL-70 and the development of lung fibrosis.24 We believe that more data is needed to confirm that these changes are clinically significant in the long-term natural history of lung disease and show that progression of the disease is indolent, but with considerable individual variability.24
Clinical improvement was found in both groups to assess dyspnea and showed similar results to those obtained by Pakas et al.8 for patients receiving high-dose cyclophosphamide and prednisone. In the Scleroderma Lung Study, a placebo-controlled, randomized double-blind trial that evaluated oral cyclophosphamide for a year, they found a similar beneficial effect on dyspnea in the group treated with cyclophosphamide.25
Both groups improved the FVC, but it was not possible to measure the diffusion capacity of carbon monoxide (DCLO). We consider this a weakness of the study. The increase in FVC above 4% in the present study is higher than reported by Simeon Aznar,26 which used pulse cyclophosphamide for 2 years and low doses of steroids. Similar results were achieved Pakas et al. in the group of high-dose prednisone. No improvement in FVC achieved clinical significance as defined by an improvement of at least 10% of the predicted value of each measurement.27 Both groups experienced improvement in the cell count of bronchoalveolar lavage after completion of treatment. The diagnosis in about 9% was of alveolitis in patients with a normal CT, close to the 10%–15% found by other authors.28 An increased percentage of neutrophils in the lavage cytology has been associated with more extensive lung disease on CT, a greater reduction in DLCO and early mortality.28 The group of low-dose prednisone is useful in the treatment of active forms of ILD, with a good safety profile and lower risk of complications secondary to the use of high doses of prednisone, such as osteoporosis, osteonecrosis, immunosuppression or the development of scleroderma renal crisis.
Although it was not the objective of this study, we evaluated the rate of skin thickness, which shows significant improvement in both groups. A similar result was obtained by Pakas et al., but only with the group of high doses of steroids. This decrease in skin thickness has been found in other studies, where the indication of cyclophosphamide was not directly related to skin involvement. However, a study by Andrade Macedo29 in Brazil, showed that the clinical form in patients with diffuse and severe skin thickening without visceral involvement had a satisfactory response to cyclophosphamide.
Unlike the results obtained by Pakas et al., our research showed that both treatment groups were favored, successful and with a good safety profile for the treatment of lung and skin involvement in systemic sclerosis. We concluded that a combination of low doses of steroids with cyclophosphamide is effective in treating ILD especially in active forms. The results show no differences from the high dose group, but the sample size and the more severe progression of patients with high doses require further studies to confirm this data.
Conflict of InterestThe authors have no disclosures to make.
Please, cite this article as: Pérez Campos D, et al. ¿ Son necesarias las dosis elevadas de prednisona para el tratamiento de la neumopatía intersticial en la esclerosis sistémica? Reumatol Clin. 2012;8(2):58–62.


