


Epidemiological information is fundamental in that it enables us to measure the importance of diseases in terms of social and public health and contributes to proper health care planning. Epidemiological studies are descriptive observational reports that provide knowledge on the disease burden in a general population, and one of their purposes is to describe the prevalence of diseases. These studies enable us to compare populations, or different moments in a given population, and thus to generate hypotheses about the possible causes of differences in the prevalences of the diseases being considered. Epidemiological analysis is of great interest not only for health care professionals, but for health care managers and financial backers. These investigations help the latter, whether they work in public administrations or in insurance companies, to estimate the expenses involved in the inclusion of novel drugs into the market.
Epidemiological studies of the musculoskeletal diseases, most of which are chronic and have a marked socioeconomic impact. Although they are associated with a high consumption of health care resources, there are few reports on them in Spain.1–3 The EPISER 2000 study,4–6 which examined the prevalence of rheumatic diseases in the Spanish adult population over 20 years of age, is 1 of the strategic projects of the Spanish Society of Rheumatology (Sociedad Española de Reumatología [SER]). The EPISER 2000 initiative was the first population-based study, a representative of the adult population in Spain, in which the authors estimated the prevalence and impact of 6 rheumatic disorders: rheumatoid arthritis, systemic lupus erythematosus, low back pain, hand and knee osteoarthritis, fibromyalgia and osteoporosis. The findings to date are considered representative of the Spanish population and are being utilized by the Spanish Ministry of Health to calculate the reimbursement corresponding to the new medications that are indicated in some of the rheumatic diseases studied.
During 2016, the SER, for different reasons, has established among its strategic objectives the conduction of a new epidemiological study of rheumatic diseases in adults, EPISER 2016. Over these last 16 years, there have been important population changes in Spain that could influence the prevalence of rheumatic diseases. According to data from the Spanish Institute of Statistics (http://www.ine.es/dynt3/inebase/es/index.htm?padre=1161&dh=1), during these years, the population over the age of 64 years has increased by 2.2%; the aging index (percentage that represents the population over the age of 64 years over that younger than 16 years) rose by 3.1%, the increase in the percentage of the foreign-born population was 5.3%, and the rates of overweight and obesity have increased by 17.6% and 3.6%, respectively (data from the 2002 Spanish National Health Survey and the 2014 European Health Interview Survey). Another important factor to be considered when talking about rheumatic disorders, especially rheumatoid arthritis, is tobacco use. According to data from the Spanish Observatory of Drugs and Drug Addiction (http://www.pnsd.msssi.gob.es/profesionales/sistemasInformacion/informesEstadisticas/pdf/ESTADISTICAS2015.pdf), during this period of time, the prevalence of the use of tobacco decreased in men in all the age groups (15–34 years and 35–64 years), whereas in women, it decreased in the first of the 2 age groups, but increased among women of 35–64 years of age (8.7%). All these changes in factors that influence rheumatic diseases clearly justify the reedition of the EPISER study.
The EPISER 2016 study will again examine, after 16 years, the prevalence of the diseases included in EPISER 2000, with the addition of others like ankylosing spondylitis, psoriatic arthritis, Sjögren's syndrome, osteoarthritis of the hip and of cervical and lumbar spine, and gout, diseases that had not been the subject of population-based studies in Spain. Moreover, as secondary objectives, EPISER 2016 will also: (a) compare the results with those obtained in EPISER 2000; (b) determine the frequency with which individuals from the Spanish adult population have seen a physician over the past year due to osteoarticular problems; and (c) establish the frequency with which Spanish adults consumed drugs for osteoarticular problems during at least 1 month over the past year.
Although the EPISER 2016 study is designed as a continuation of EPISER 2000, there are differences between the 2 reports: (1) the new study will examine the prevalence of a greater number of rheumatic diseases; (2) more classification and diagnostic criteria will be used; (3) the sample size will duplicate that of the anterior study; and (4) recruitment will be done differently.
To compare the 2 studies, the same classification criteria of EPISER 2000 will be used but, in addition, we will include the new classification criteria that have been incorporated in recent years. For example, in rheumatoid arthritis, we will have the 1987 American College of Rheumatology (ACR) criteria (used in EPISER 2000), as well as the new 2010 criteria for ACR/European League Against Rheumatism (EULAR).
A sample size of 5000 individuals was estimated for the EPISER 2016 study, assuming a Poisson distribution, to obtain a 95% confidence interval of 0.3–0.77 for an expected prevalence of rheumatoid arthritis of 0.5%, and a 95% confidence interval of 0.14–0.54 for an expected prevalence of psoriatic arthritis of 0.3%. In EPISER 2000, the sample size was 2998 individuals, with a final number of 2192 interviews. The larger sample size in EPISER 2016 will confer greater precision for determining the true prevalence of the diseases being studied.
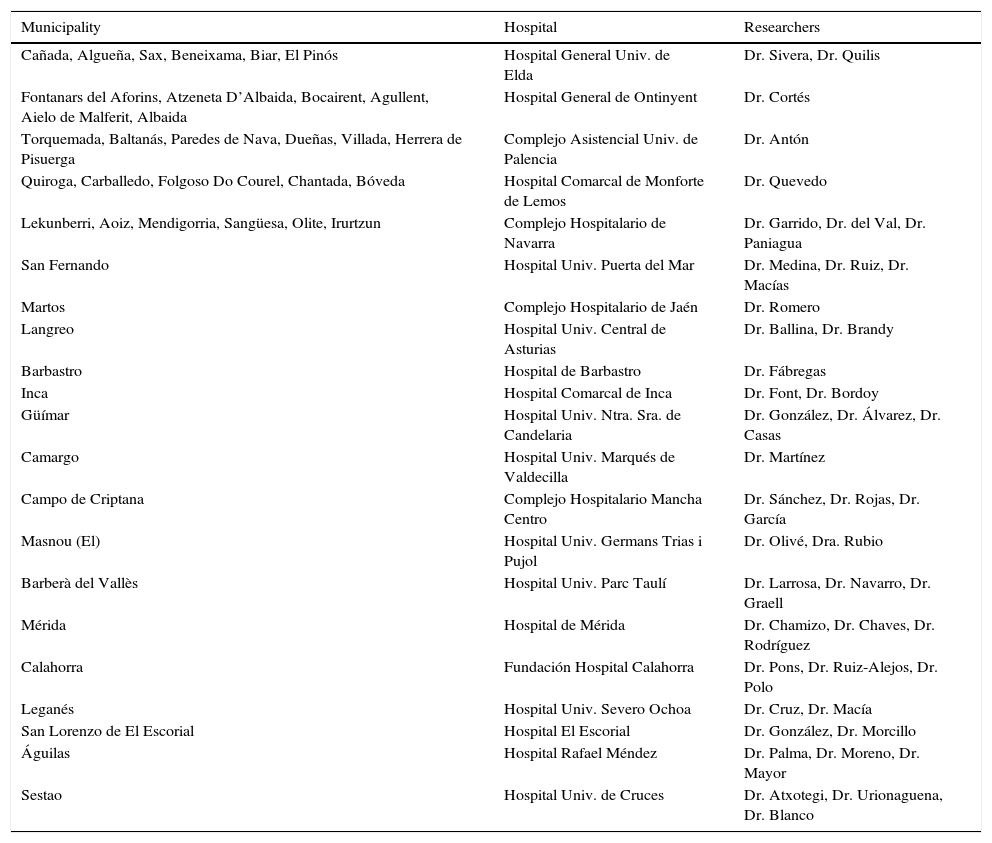
As in EPISER 2000, the sample will be selected by stratified multistage cluster and by conglomerates. Stratification was done by age and sex in blocks of 10 years, in accordance with the distribution of the Spanish population, the rural/urban nature of the municipalities and autonomous communities. In the present study, participation will come from 45 municipalities (see Table 1) from 17 autonomous communities.
Hospitals participating in EPISER 2016.
| Municipality | Hospital | Researchers |
|---|---|---|
| Cañada, Algueña, Sax, Beneixama, Biar, El Pinós | Hospital General Univ. de Elda | Dr. Sivera, Dr. Quilis |
| Fontanars del Aforins, Atzeneta D’Albaida, Bocairent, Agullent, Aielo de Malferit, Albaida | Hospital General de Ontinyent | Dr. Cortés |
| Torquemada, Baltanás, Paredes de Nava, Dueñas, Villada, Herrera de Pisuerga | Complejo Asistencial Univ. de Palencia | Dr. Antón |
| Quiroga, Carballedo, Folgoso Do Courel, Chantada, Bóveda | Hospital Comarcal de Monforte de Lemos | Dr. Quevedo |
| Lekunberri, Aoiz, Mendigorria, Sangüesa, Olite, Irurtzun | Complejo Hospitalario de Navarra | Dr. Garrido, Dr. del Val, Dr. Paniagua |
| San Fernando | Hospital Univ. Puerta del Mar | Dr. Medina, Dr. Ruiz, Dr. Macías |
| Martos | Complejo Hospitalario de Jaén | Dr. Romero |
| Langreo | Hospital Univ. Central de Asturias | Dr. Ballina, Dr. Brandy |
| Barbastro | Hospital de Barbastro | Dr. Fábregas |
| Inca | Hospital Comarcal de Inca | Dr. Font, Dr. Bordoy |
| Güímar | Hospital Univ. Ntra. Sra. de Candelaria | Dr. González, Dr. Álvarez, Dr. Casas |
| Camargo | Hospital Univ. Marqués de Valdecilla | Dr. Martínez |
| Campo de Criptana | Complejo Hospitalario Mancha Centro | Dr. Sánchez, Dr. Rojas, Dr. García |
| Masnou (El) | Hospital Univ. Germans Trias i Pujol | Dr. Olivé, Dra. Rubio |
| Barberà del Vallès | Hospital Univ. Parc Taulí | Dr. Larrosa, Dr. Navarro, Dr. Graell |
| Mérida | Hospital de Mérida | Dr. Chamizo, Dr. Chaves, Dr. Rodríguez |
| Calahorra | Fundación Hospital Calahorra | Dr. Pons, Dr. Ruiz-Alejos, Dr. Polo |
| Leganés | Hospital Univ. Severo Ochoa | Dr. Cruz, Dr. Macía |
| San Lorenzo de El Escorial | Hospital El Escorial | Dr. González, Dr. Morcillo |
| Águilas | Hospital Rafael Méndez | Dr. Palma, Dr. Moreno, Dr. Mayor |
| Sestao | Hospital Univ. de Cruces | Dr. Atxotegi, Dr. Urionaguena, Dr. Blanco |
The recruitment of the population selected in EPISER 2000 was done by informative letters and by telephone. The rheumatologist was responsible for making the call and the subsequent interview. In EPISER 2016, the telephone calls will be done with the participation of an outside company devoted to sociological studies with experience in the health field (IPSOS), and a computer-assisted telephone interviewing (CATI) call center service. An ad hoc telephone survey will be conducted to identify patients who might have the disorders studied. The survey will be divided into the following blocks of questions: sociodemographic, general health status, use of tobacco, rheumatic disease screening and variables related to the use of health resources for osteoarticular problems (medical appointments and medications). The confirmation of questionnaires with positive screening will be done by a rheumatologist, on the basis of other validated diagnostic criteria. The specialist will contact these individuals to confirm the suspected diagnosis and schedule a physical examination and the following ancillary tests: sacroiliac radiographs and human lymphocyte antigen (HLA) B27, for ankylosing spondylitis; complete blood count, rheumatoid factor, anti-cyclic citrullinated peptide antibodies, erythrocyte sedimentation rate, reactive-C protein, and plain radiographs of feet and hands, for rheumatoid arthritis; rheumatoid factor and plain radiographs of hands and feet, for psoriatic arthritis; serum uric acid and plain radiographs of hands and feet, for gout; complete blood count, antinuclear antibodies, anti-double stranded [ds]DNA and urinary sediment, for systemic lupus erythematosus; antinuclear antibodies, anti-SSA/Ro and SSB/La antibodies and rheumatoid factor, for Sjögren's syndrome; hip radiographs, for hip osteoarthritis; radiographs of knees, cervical spine and lumbar spine, for knee and cervical and lumbar spine osteoarthritis, respectively; and complete blood count, laboratory tests and thyroid hormones, for fibromyalgia.
One of the possible limitations to EPISER 2016 is the potential selection bias introduced by the fact of using the landline telephone as a recruitment tool. According to the data from the study by García-Continente et al.,7 persons with access only to a mobile phone were probably from a manual social class, had a lower educational level, born outside of Spain and smokers. Of these variables, tobacco use is a recognized risk factor for some of the diseases in this study. Thus, during recruitment, an intermediate analysis will be performed to determine the proportion of smokers in the sample. If, in this analysis, we detect a particular difference with respect to the proportion of smokers in Spain (according to the 2014 European Health Interview Survey), it will be taken into account in recruitment from that time on, so that the difference will not be apparent in the final sample. This same strategy will be used for the relationship “born in Spain/born outside of Spain”, taking as a reference the ongoing population census from the web page of the Spanish Institute of Statistics (http://www.ine.es/inebmenu/mnupadron.htm). On the other hand, prior to beginning the study, the comparison will be made between the number of landline phones available and the number of homes in each municipality, according to the latest population census.
The EPISER 2016 study was funded by different drug companies and by the SER. The project was approved by the clinical research ethics committees of the participating hospitals, and telephone recruiting began at the end of November. There is a notable campaign to spread the information to the populations of the municipalities included by means of posters in town halls and health centers, announcements by the press and interviews broadcast by local radio stations. We hope that the initial results will be available by the first third of 2018. We are completely convinced that the results of EPISER 2016 will lead to a better knowledge of the true prevalence of the major musculoskeletal diseases affecting the Spanish population.
To Daniel Seoane, Carlos Sánchez-Piedra, Jesús Sánchez and Fernando Alonso, members of the research unit of the SER, for the work they are doing to ensure that EPISER 2016 is a success. To Dr. Fernando Pérez Ruiz, Lucía Silva Fernández, José María Pego Reigosa, Francisca Sivera Mascaró, Francisco Javier Blanco García, Francisco Javier Narváez García and Antonio Juan Mas, members of the scientific committee, and to Dr. Javier Llorca, an outside assessor for EPISER 2016.
Please cite this article as: Bustabad S, Díaz-González F. Estudio EPISER 2016. El porqué de un nuevo estudio epidemiológico. Reumatol Clin. 2017;13:1–3.


