

Ankylosing spondylitis (AS) is a chronic inflammatory disease that mainly affects the axial skeleton and, to a lesser degree, the appendicular skeleton. The shoulder is the second most frequently affected multiaxial joint in AS.1 Of all the inflammatory arthropathies, it is the least erosive and the most ossifying; its predominant feature is joint ankylosis.2 We present the case of a patient who experienced destructive and nondestructive changes in the shoulder joint.
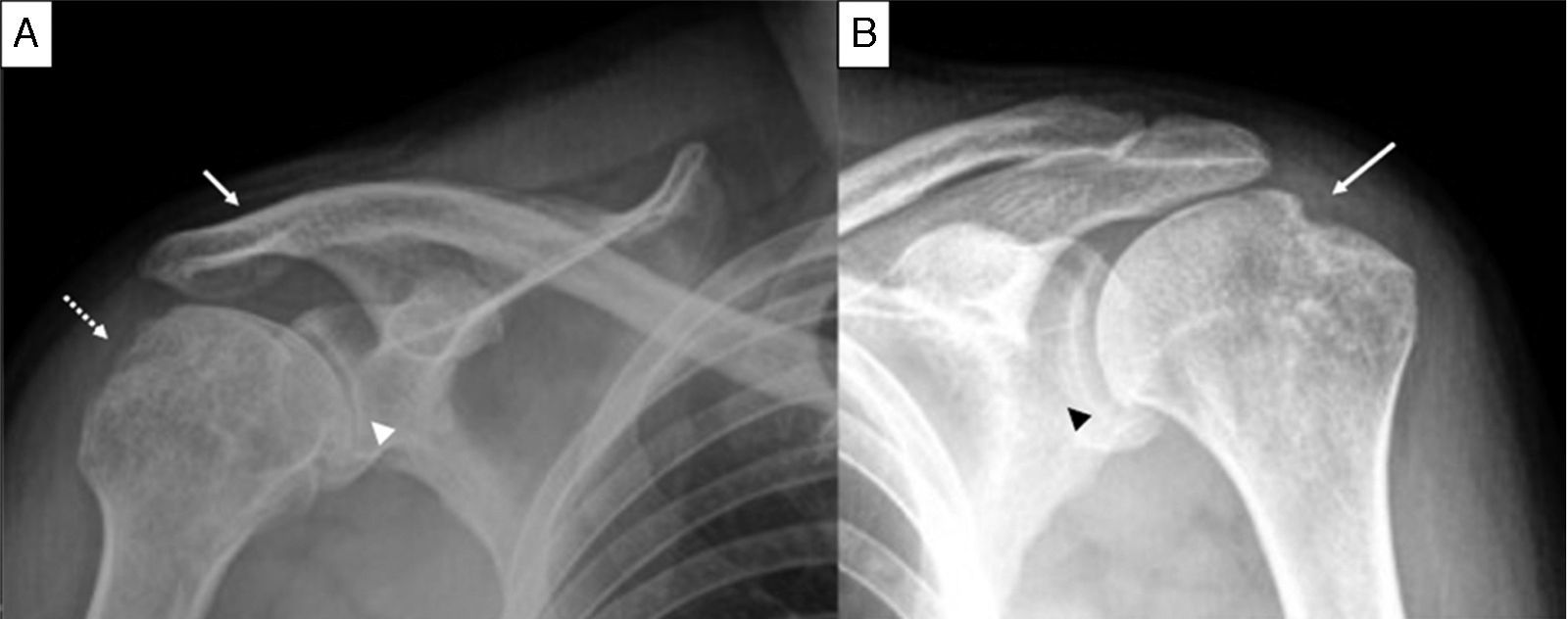
The patient was a 36-year-old man, who had had inflammatory low back pain since the age of 16 years. His low back and neck mobility was limited, he had arthritis of the thighs, ankles and shoulders, and was HLA-B27-positive. At the age of 23 years, he required bilateral hip replacement. He presented with a 1-year history of disability involving the movement of his shoulders, predominantly the right. Physical examination revealed limitation of the ranges of mobility for flexion, extension and abduction. The radiographic findings were bilateral grade II sacroiliitis in pelvis, and squaring of the vertebral bodies and vertebral ankylosis from T11 to L2 in lumbar spine. Right shoulder had degenerative changes, erosions and ankylosis of the acromioclavicular joint (Fig. 1A); left shoulder showed a narrowing of the glenohumeral joint space, erosion in the greater tuberosity of the humerus and degenerative changes (Fig. 1B).
 The view of right shoulder shows erosions in the greater tuberosity (dashed arrow), narrowing of the glenohumeral joint space (arrowhead) and ankylosis of the acromioclavicular joint (arrow). (B) The view of left shoulder shows narrowing of the glenohumeral joint space (arrowhead) and the hatchet sign (arrow).")
Anteroposterior projection of shoulders. (A) The view of right shoulder shows erosions in the greater tuberosity (dashed arrow), narrowing of the glenohumeral joint space (arrowhead) and ankylosis of the acromioclavicular joint (arrow). (B) The view of left shoulder shows narrowing of the glenohumeral joint space (arrowhead) and the hatchet sign (arrow).
Among the spondyloarthritides, psoriatic arthritis and AS are those that most frequently affect the glenohumeral joint.1 At the present time, enthesitis is widely recognized as a feature of AS. In the ultrasound evaluation of the shoulder in individuals with AS, enthesitis constitutes the most common disorder (56.6%), mainly affecting the supraspinatus and subscapularis tendons, whereas involvement of the acromioclavicular joint is not reported.3 Plain radiography is one of the most widely employed imaging techniques. Three disease processes are the basis of the radiographic signs: inflammation, bone repair and ossification. Two types of involvement have been described in shoulder: the nondestructive form is characterized by a humeral head ankylosed to the glenoid and considerable ossification of the coracoclavicular ligament; the destructive form, which is less common, is described as erosion of the humeral head, which becomes hatchet-shaped, the “hatchet” sign.1,2 In radiographic studies, the acromioclavicular joint is the most common site of shoulder involvement in AS, and the changes most frequently are degenerative.3,4 To the best of our knowledge, prior to the case we describe here, another 2 cases of AS with acromioclavicular ankylosis were reported.5,6 Enthesitis involving the acromioclavicular joint may lead to its ankylosis. Thus, patients with long-standing AS and hip involvement should have the status of their shoulders evaluated.
Ethical DisclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingThe authors declare that they have received no funding for the performance of the work for this report.
Conflicts of InterestThe authors declare they have no conflicts of interest.
Please cite this article as: Horta-Baas G, Jiménez-Balderas FJ. Hallazgos radiográficos de la afectación del hombro en espondilitis anquilosante. Reumatol Clin. 2016;12:296–297.


