


To determine the cost of medical care in patients with gonarthrosis.
Material and methodsCost study in patients over 40 years of age with gonarthrosis, diagnosed according to the radiological classification of Kellgren and Lawrence. The average annual cost (euros) was estimated taking the unit cost plus average use of services such as family medicine, imaging, laboratory, electrodiagnosis, orthopaedics, hospitalisation, physical therapy, surgery, nutrition, preoperative assessment and medication. Projections based on assumptions were made for three scenarios.
ResultsGrade 2 gonarthrosis predominated at 39.7% (95% confidence interval, 33.8–45.6). The annual cost of care for a patient with gonarthrosis was €108.87 in the intermediate scenario, €86.73 in the lower cost scenario and €132.60 in the higher cost scenario. For a population of 119,530,753 inhabitants, with 10,937,064 gonarthrosis patients, the annual cost in the intermediate scenario was €1,190,685,273 and represented 4.48% of the health expenditure.
ConclusionThe average annual cost of gonarthrosis is relatively low, but when related to prevalence and prevalence trends, it can become a serious problem for health services.
Determinar el costo de la atención médica en pacientes con gonartrosis.
Material y métodosEstudio de costos en pacientes mayores de 40 años con diagnóstico de gonartrosis realizado de acuerdo a la clasificación radiológica de Kellgren y Lawrence. El costo promedio anual (euros) construido a partir del costo unitario y el uso promedio se estimó para medicina familiar, pruebas de imagen, laboratorio, electrodiagnóstico, ortopedia, hospitalización, terapia física, quirófano, nutrición, valoración prequirúrgica y medicamentos. Se realizaron proyecciones basadas en supuestos para 3 escenarios.
ResultadosPredomina el grado 2 de gonartosis con 39,7% (IC 95%; 33,8-45,6). El costo anual de la atención del paciente con gonartrosis en el escenario promedio es 108.87 euros (€), en el escenario bajo 86.73€ y en el escenario alto 132.60€.
Para una población de 119.530.753 habitantes, con 10.937.064 pacientes que cursan con gonartrosis, el costo anual en el escenario promedio es 1.190.685.273€ y representa el 4,48% del gasto en salud.
ConclusiónEl costo promedio anual de la gonartrosis es relativamente bajo, pero al relacionarlo con la prevalencia y la tendencia de la prevalencia se puede convertir en un serio problema para los servicios de salud.
Osteoarthrosis is a public health problem due to its prevalence, the degree of disability that it generates in the population, and its cost for health services.1
Its prevalence has been reported at between 25% and 30% in the population aged from 45 to 65, but has been highlighted at 85% in those aged over 65.2–5 By contrast, other studies show lower percentages, between 2.3% and 11%.6,7
The knee in particular (gonoarthritis) is the most prone to osteoarthrosis due to trauma, and accidental or repetitive injury in the form of wear and tear.8
The literature notes that trends are on the rise. The condition is expected to increase to 52% by 2040 due to ageing and obesity9; in countries such as Mexico it has been suggested that the total number of patients with gonarthrosis will reach 20 million by 2050.10
Diagnosis of gonarthrosis is based on radiological findings, and the Kellgren and Lawrence scale is used most to evaluate structural damage.11,12
The treatment approach is multidisciplinary and favours analgesia, limitation of disability and improving joint function. Pharmacological treatment has a broad therapeutic arsenal, and rehabilitation based on education and isometric and isotonic exercises has proved useful. In addition, surgical management includes arthroscopy and total arthroplasty.13,14
Usage of the health services by patients with gonarthrosis is increasing, as are the costs and loss of productivity generated. It has been highlighted that in countries like France, direct annual costs have risen to 4.5 million francs. In Spain the annual cost is €26,579.5.15,16
Most studies on the costs relating to gonarthrosis have been performed concerning the cost of replacement surgery, and reports place this at €7645.17
The condition has also been compared with more severe diseases such as rheumatoid arthritis, and the cost has turned out to be higher in line with higher prevalence.18,19
In Latin America, costs studies tend to focus on the cost-effectiveness of treatment, leaving the dimension of costs uncovered. However, there are studies on the subject20,21 that definitely require complementing, and therefore the aim of this article is to determine the medical care costs of patients with gonarthrosis.
Material and methodsA study was undertaken of the costs in patients over the age of 40 with a diagnosis of gonarthrosis, belonging to a social security institution in Querétaro, México.
The information was analysed from medical records from January to December 2016.
Patients with any grade of gonarthrosis were included, and the diagnosis was made according to Kellgren and Lawrence's radiological classification.
Sociodemographic variables (age, sex, occupation), and clinical characteristics (grade of gonarthrosis according to Kellgren and Laurence's radiological classification, body mass index, nutritional status using BMI as the benchmark).
Average costThe average annual cost (Euros) was estimated for family medicine, imaging tests, laboratory, electrodiagnosis, orthopaedics, hospitalisation, physiotherapy, operating room, nutrition, preoperative assessment and medication.
The product of 2 variables, usage profile and unit cost, was used to determine annual costs.
Usage profileMedical records that noted the type of service used and the intensity of use over one year were reviewed to determine the usage profile.
In order to determine the total number of medical records to study, we calculated the sample size (n=262) with the formula of finite population percentages (n=9000), 95% confidence level for a tail (z=1.64), average usage of family medicine services of 5.6 services per year, standard deviation .5 and margin of error .05.
Simple random sampling was used to determine the medical records for inclusion, using the nominal list of the population with a diagnosis of gonarthrosis in the medical unit as the sample framework.
The services analysed included family practice, imaging tests, laboratory, electrocardiography, orthopaedics, hospitalisation, intensive therapy, operating room, nutrition, preoperative assessment and medication.
Unit costThe unit cost integrated the fixed unit cost and the variable unit cost.
The fixed unit cost. The fixed unit cost was calculated using the time and motion technique.
- •
For this purpose, the quantity of human inputs, equipment, furniture, instruments and basic services (water, electricity, telephone, fuel) was identified in each of the services covered.
- •
In parallel, the unit cost per input (information obtained from existing payroll receipts and records in the administrative department of the medical unit).
- •
The value obtained was divided between the total days worked per year, and thus the daily expenditure was identified.
- •
The daily expenditure was divided among the total patients attended per day (information taken from the daily productivity report), and thus the fixed unit cost per input was obtained.
- •
The sum of the fixed unit costs per input enabled the fixed unit cost to be determined.
Variable unit cost. The variable unit cost was determined using the microcosting technique.
- •
The amount of inputs per type of care (medication, dressing materials) was identified in the medical record.
- •
The cost of each input was obtained from the institutional office in charge of input purchasing.
- •
The amount of inputs per type of care was multiplied by the cost of each input and the variable unit cost per input was obtained.
- •
The sum of the variable unit costs per input enabled identification of the variable unit cost per type of care.
The average cost per service was obtained by adding the unit cost per input of all the inputs of the service.
Total average costThe sum of the average costs per service enabled identification of the total average cost per patient.
The unit cost per input was obtained by adding the fixed unit cost and the variable unit cost of each input.
ProjectionsThe total cost for a given population was projected based on the total average cost per patient, assuming that the prevalence of the population aged over 40 is 30.5% and the prevalence of gonarthrosis in over 40-year-olds is 30%.
Two extreme cost scenarios were considered, low and high, using the confidence interval as the point of reference for the usage profile.
ResultsThe average age of the population studied was 58.38 years (95%CI: 57.03–59.74), females predominated at 61.3% (95%CI: 55.4–67.2), the main occupation was housewife in 41.5% (95%CI: 35.5–47.5), the average body mass index was 30.49 (95%CI: 29.49–30.67), the prevalence of excess weight was 43.7% (95%CI: 37.7–49.7), and the prevalence of obesity 42.3% (95%CI: 36.3–48.3).
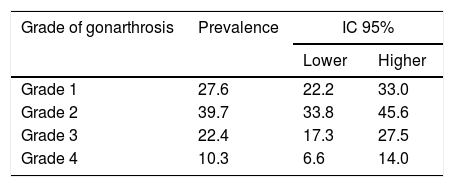
In the population studied, grade 2 gonarthrosis predominated at 39.7% (95%CI: 33.8–45.6). The rest of the information is shown in Table 1.
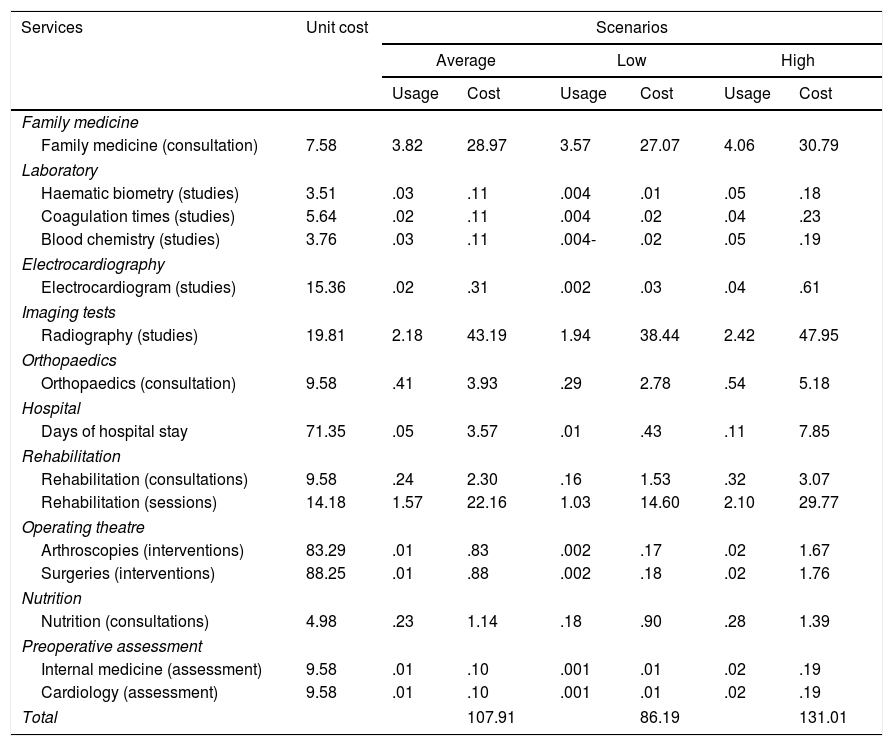
The highest unit cost was for surgery performed in the operating theatre €88.25. The service with the highest usage was family medicine at 3.82 consultations per year, in the average scenario the total cost was €10,791, in the low scenario €86.19, and in the high scenario €13,101. Table 2 shows the usage and costs per service and type of scenario.
Average usage, unit cost and average cost per service, input and scenario type.
| Services | Unit cost | Scenarios | |||||
|---|---|---|---|---|---|---|---|
| Average | Low | High | |||||
| Usage | Cost | Usage | Cost | Usage | Cost | ||
| Family medicine | |||||||
| Family medicine (consultation) | 7.58 | 3.82 | 28.97 | 3.57 | 27.07 | 4.06 | 30.79 |
| Laboratory | |||||||
| Haematic biometry (studies) | 3.51 | .03 | .11 | .004 | .01 | .05 | .18 |
| Coagulation times (studies) | 5.64 | .02 | .11 | .004 | .02 | .04 | .23 |
| Blood chemistry (studies) | 3.76 | .03 | .11 | .004- | .02 | .05 | .19 |
| Electrocardiography | |||||||
| Electrocardiogram (studies) | 15.36 | .02 | .31 | .002 | .03 | .04 | .61 |
| Imaging tests | |||||||
| Radiography (studies) | 19.81 | 2.18 | 43.19 | 1.94 | 38.44 | 2.42 | 47.95 |
| Orthopaedics | |||||||
| Orthopaedics (consultation) | 9.58 | .41 | 3.93 | .29 | 2.78 | .54 | 5.18 |
| Hospital | |||||||
| Days of hospital stay | 71.35 | .05 | 3.57 | .01 | .43 | .11 | 7.85 |
| Rehabilitation | |||||||
| Rehabilitation (consultations) | 9.58 | .24 | 2.30 | .16 | 1.53 | .32 | 3.07 |
| Rehabilitation (sessions) | 14.18 | 1.57 | 22.16 | 1.03 | 14.60 | 2.10 | 29.77 |
| Operating theatre | |||||||
| Arthroscopies (interventions) | 83.29 | .01 | .83 | .002 | .17 | .02 | 1.67 |
| Surgeries (interventions) | 88.25 | .01 | .88 | .002 | .18 | .02 | 1.76 |
| Nutrition | |||||||
| Nutrition (consultations) | 4.98 | .23 | 1.14 | .18 | .90 | .28 | 1.39 |
| Preoperative assessment | |||||||
| Internal medicine (assessment) | 9.58 | .01 | .10 | .001 | .01 | .02 | .19 |
| Cardiology (assessment) | 9.58 | .01 | .10 | .001 | .01 | .02 | .19 |
| Total | 107.91 | 86.19 | 131.01 | ||||
The cost is expressed in Euros.
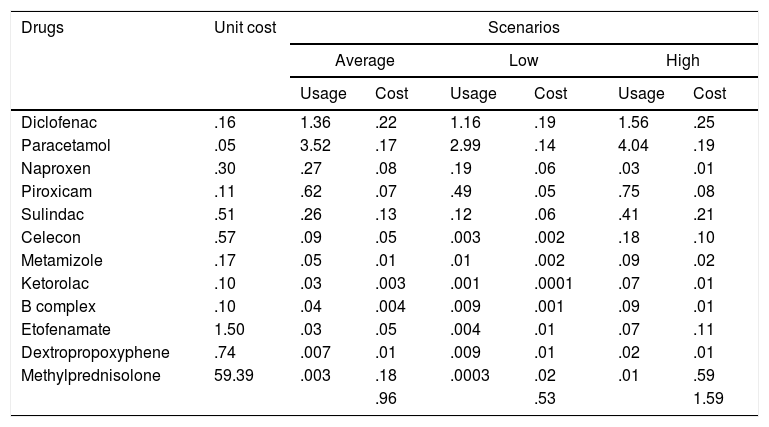
The highest unit cost was for methylprednisolone (€59.39), the cost in the average scenario was €.96. Table 3 shows the usage, cost per drug, and total cost per scenario.
Average usage, unit cost and average cost per drug type and scenario type.
| Drugs | Unit cost | Scenarios | |||||
|---|---|---|---|---|---|---|---|
| Average | Low | High | |||||
| Usage | Cost | Usage | Cost | Usage | Cost | ||
| Diclofenac | .16 | 1.36 | .22 | 1.16 | .19 | 1.56 | .25 |
| Paracetamol | .05 | 3.52 | .17 | 2.99 | .14 | 4.04 | .19 |
| Naproxen | .30 | .27 | .08 | .19 | .06 | .03 | .01 |
| Piroxicam | .11 | .62 | .07 | .49 | .05 | .75 | .08 |
| Sulindac | .51 | .26 | .13 | .12 | .06 | .41 | .21 |
| Celecon | .57 | .09 | .05 | .003 | .002 | .18 | .10 |
| Metamizole | .17 | .05 | .01 | .01 | .002 | .09 | .02 |
| Ketorolac | .10 | .03 | .003 | .001 | .0001 | .07 | .01 |
| B complex | .10 | .04 | .004 | .009 | .001 | .09 | .01 |
| Etofenamate | 1.50 | .03 | .05 | .004 | .01 | .07 | .11 |
| Dextropropoxyphene | .74 | .007 | .01 | .009 | .01 | .02 | .01 |
| Methylprednisolone | 59.39 | .003 | .18 | .0003 | .02 | .01 | .59 |
| .96 | .53 | 1.59 | |||||
The cost is expressed in Euros.
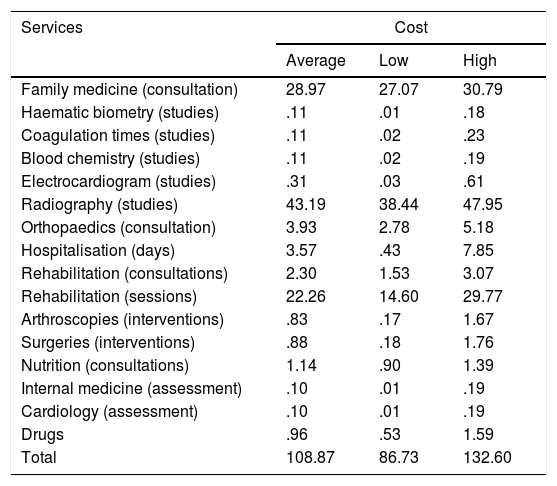
The annual cost of the care of patients with gonarthrosis in the high scenario was €132.60 and in the average scenario €108.87. Table 4 shows the costs per service, and per type of scenario.
Average cost per service and institution and total cost per scenario.
| Services | Cost | ||
|---|---|---|---|
| Average | Low | High | |
| Family medicine (consultation) | 28.97 | 27.07 | 30.79 |
| Haematic biometry (studies) | .11 | .01 | .18 |
| Coagulation times (studies) | .11 | .02 | .23 |
| Blood chemistry (studies) | .11 | .02 | .19 |
| Electrocardiogram (studies) | .31 | .03 | .61 |
| Radiography (studies) | 43.19 | 38.44 | 47.95 |
| Orthopaedics (consultation) | 3.93 | 2.78 | 5.18 |
| Hospitalisation (days) | 3.57 | .43 | 7.85 |
| Rehabilitation (consultations) | 2.30 | 1.53 | 3.07 |
| Rehabilitation (sessions) | 22.26 | 14.60 | 29.77 |
| Arthroscopies (interventions) | .83 | .17 | 1.67 |
| Surgeries (interventions) | .88 | .18 | 1.76 |
| Nutrition (consultations) | 1.14 | .90 | 1.39 |
| Internal medicine (assessment) | .10 | .01 | .19 |
| Cardiology (assessment) | .10 | .01 | .19 |
| Drugs | .96 | .53 | 1.59 |
| Total | 108.87 | 86.73 | 132.60 |
The cost is expressed in Euros.
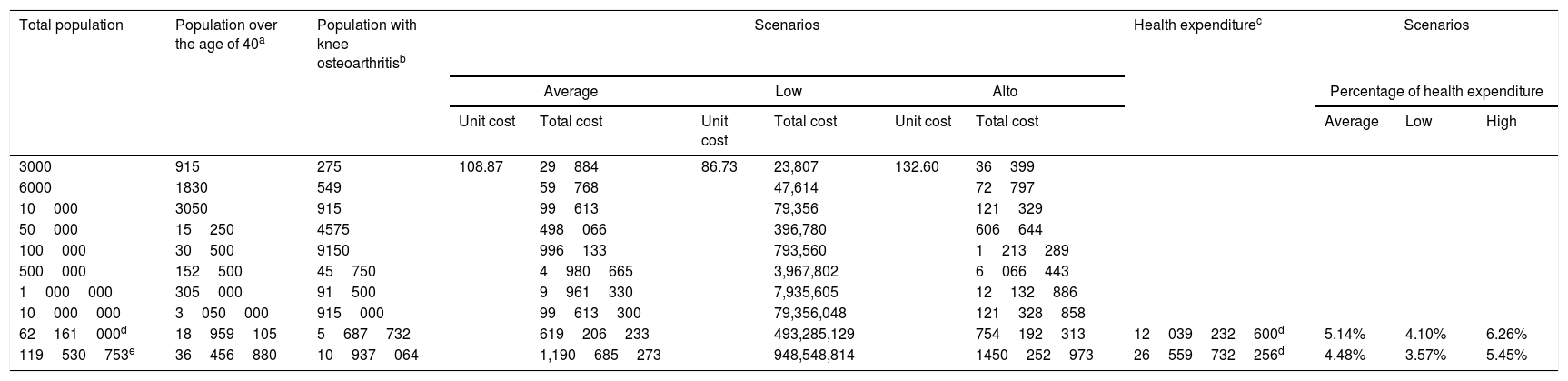
For a population of 119,530,753 inhabitants, of whom 31% were aged 40 or more (36,456,880), and of these 10,937,064 had gonarthrosis, the annual cost in the average scenario was 1,190,685,273€, and represented 4.48% of health expenditure. Table 5 shows the cost for the low scenario and for the high scenario; it also shows the costs for different populations.
Cost projection per scenario type and total population. Percentage of health expenditure.
| Total population | Population over the age of 40a | Population with knee osteoarthritisb | Scenarios | Health expenditurec | Scenarios | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Average | Low | Alto | Percentage of health expenditure | |||||||||
| Unit cost | Total cost | Unit cost | Total cost | Unit cost | Total cost | Average | Low | High | ||||
| 3000 | 915 | 275 | 108.87 | 29884 | 86.73 | 23,807 | 132.60 | 36399 | ||||
| 6000 | 1830 | 549 | 59768 | 47,614 | 72797 | |||||||
| 10000 | 3050 | 915 | 99613 | 79,356 | 121329 | |||||||
| 50000 | 15250 | 4575 | 498066 | 396,780 | 606644 | |||||||
| 100000 | 30500 | 9150 | 996133 | 793,560 | 1213289 | |||||||
| 500000 | 152500 | 45750 | 4980665 | 3,967,802 | 6066443 | |||||||
| 1000000 | 305000 | 91500 | 9961330 | 7,935,605 | 12132886 | |||||||
| 10000000 | 3050000 | 915000 | 99613300 | 79,356,048 | 121328858 | |||||||
| 62161000d | 18959105 | 5687732 | 619206233 | 493,285,129 | 754192313 | 12039232600d | 5.14% | 4.10% | 6.26% | |||
| 119530753e | 36456880 | 10937064 | 1,190685273 | 948,548,814 | 1450252973 | 26559732256d | 4.48% | 3.57% | 5.45% | |||
The cost is expressed in Euros.
Gonarthrosis can be considered a chronic degenerative disease that requires health services on a permanent basis, and from this perspective inputs are required to generate care, resources that are scarce in the current health economy.22 In this scenario it is important to identify the inputs required to provide care, and hence the importance of this article.
In this article, construction of the average cost covers 2 dimensions, usage profile and cost, each of them with its own methodology, and this scenario can be considered a strength of the study that supports the data presented.
It is true that the reported cost is the average, an estimator considered fixed, but it is also true that when the high and low scenarios are presented, the possibilities of information widen, and therefore the value presented takes on another dimension. However, when this is interpreted it must be borne in mind that the scenarios were estimated according to the usage profile of the health services, and that this same estimate might have the unit cost as the benchmark.
In this paper, although about costs, we covered the epidemiological dimension, therefore when adopting the total average cost it should be borne in mind that this is the cost of a population with gonarthrosis, according to the prevalence of the grades of gonarthrosis presented, and that it could be very different to another population in which the prevalence by grade were different.
It is true that the results express a very low cost for medication; there could be 2 explanations for this: it is a reality that the consolidated purchases of the public institutions are reflected in a low unit cost and impact the average cost, this amount compared with the market price reflects a huge difference, but it is a reality that cannot be refuted. If the article had proposed a comparison between public and private institutions, the difference in cost would have been marked by a ratio of 5 units or more. Furthermore, by analysing the average cost expressed for drugs it should be borne in mind that this refers to the average, which means that the same drug is not prescribed to the entire population, and therefore the value calculated is estimated in terms of the total number of patients studied, hence the value reported.
The average cost reported for gonarthrosis, and the cost for the low and high scenario is lower than those reported for the care of chronic diseases such as diabetes or hypertension. It should also be noted that the costs of these diseases correspond to care provided at the first level of care, while the cost of gonarthrosis includes all services generated throughout the natural course of the disease.
It seems logical that of all the services employed radiology contributes most to the average cost, since radiological assessment is the benchmark for determining the progress, and for monitoring patients with gonarthrosis. This does not mean that the cost of surgery is not high, it is, but as a unit cost. However, it is also true that few among this population undergo a surgical procedure, therefore in the end it is not the most significant service for integrating costs.
In conclusion, it can be said that the average annual cost of gonarthrosis is relatively low, but when related to prevalence and prevalence trends it could become a serious problem for the health services.
Conflict of interestsThe authors have no conflict of interests to declare
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have adhered to the protocols of their centre of work on patient data publication.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Please cite this article as: Villarreal-Ríos E, Cedillo-García M, Vargas-Daza ER, Galicia-Rodríguez L, Martínez-González L, Escorcia-Reyes V. Costo directo de la atención médica en pacientes con gonartrosis. Reumatol Clin. 2019;15:277–281.


