

An 83-year-old male with a 2-history of right hip pain. Initial examination showed moderate pain on palpation of the right trochanteric region with no phlogistic signs and no limitation of joint range. With an initial diagnosis of trochanteric bursitis, treatment with oral anti-inflammatories was initiated. Due to persistent pain, glucocorticoid injection was given. However, the symptoms persisted, and functional limitation was evident months following onset.
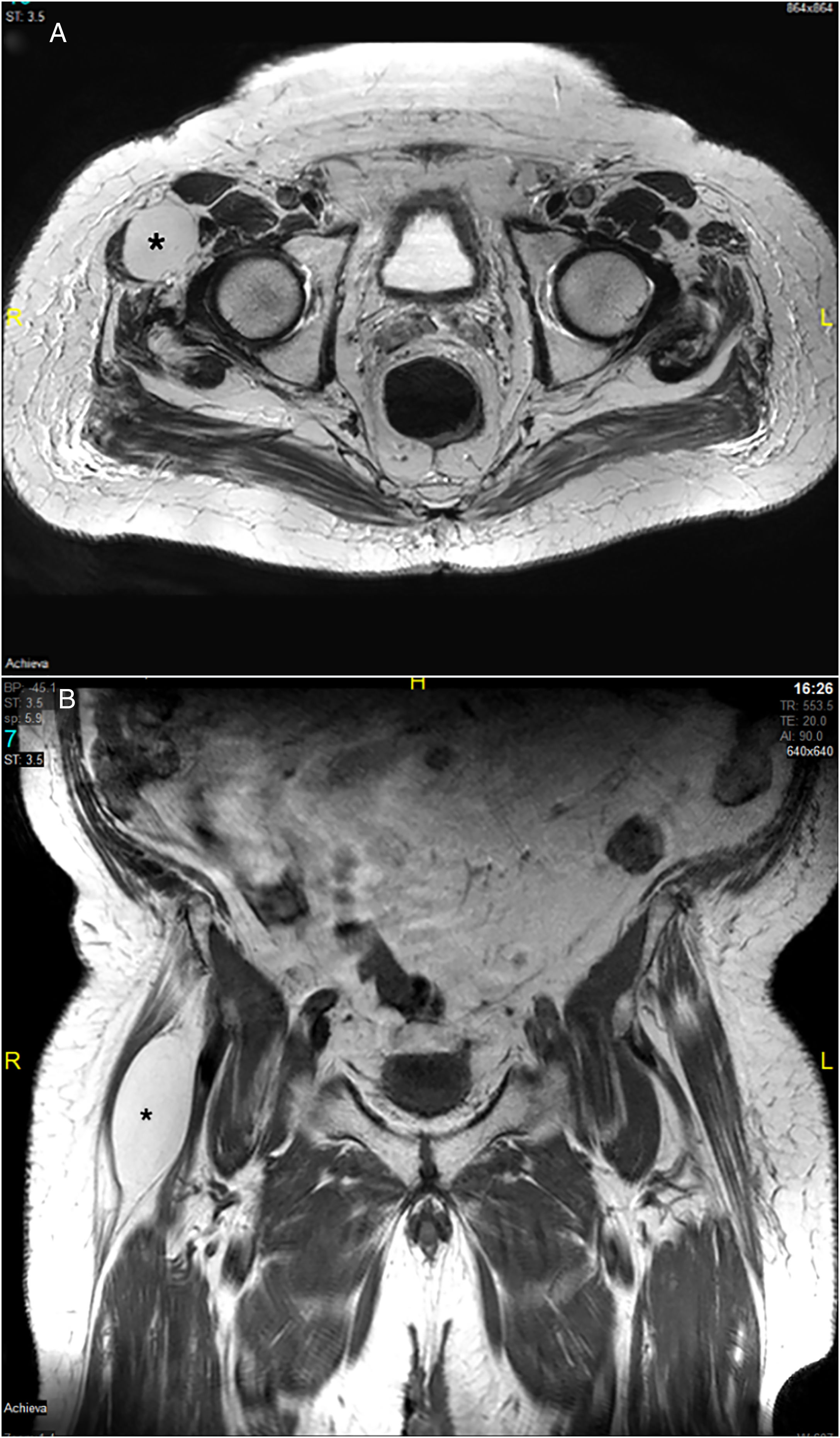
Reassessment showed pain on palpation of moderate-severe intensity together with a hard, non-stony tumor with flogotic signs seated on the upper third of the lateral face of the affected limb. An MRI of both hips was requested (Fig. 1), which showed edema in the soft tissues around the right greater trochanter, compatible with enthesitis, as well as a well-defined ovoid lesion, 42mm×38mm×77mm, located in the deep plane between the belly of the tensor muscle of the fascia lata and the sartorius muscle. Biopsy showed multiple foci of steatonecrosis with associated xanthomatous reaction. The lesion was surgically removed, with good clinical outcome.
 between the belly of the fascia lata tensor muscle and the sartorius muscle. (A) Hip MRI, axial plane. (B) Hip MRI, coronal plane.")
The latent clinical course and slow growth of the tumor could discourage the physician from suspecting a pathology with potential risk.1–4 However, persistent unilateral pain, in the absence of other factors, should alert suspicion of an unusual pathology.5–7 In this regard, the frequency of intramuscular lipomas is approximately 0%–5%, and .3%–1.9% for intermuscular lipomas, the most common location being the thigh.8–10 Our case highlights the importance of confirming the nature of any soft tissue inflammatory process with additional imaging tests and biopsy, if necessary.
FundingThe authors declare that they have received no funding for this paper.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Vílchez-Oya F, Salman-Monte TC, Monfort J. Dolor de cadera secundario a lipoma intermuscular. Reumatol Clin. 2021;17:175–177.


