


To describe the methodology of REAPSER (Spanish Registry of Recent-onset Psoriatic Arthritis), its strengths and limitations. The aim of this study is to identify prognostic factors for the clinical and radiographic course in a cohort of patients with psoriatic arthritis (PsA) diagnosed within 2years of symptom evolution.
MethodsMulticenter, observational and prospective study (with 2-year follow-up including annual visits). Baseline visit intended to reflect patient situation before the disease course was modified by treatments prescribed in rheumatology departments. Patients were invited to participate consecutively in one of their routine visits to the rheumatologist. 211 patients were included. Following data were collected: sociodemographic variables; employment situation; family history; personal history and comorbidities; anthropometric data; lifestyle; use of healthcare services; clinical situation at the time of PsA diagnosis; joint involvement and spinal pain; pain and overall assessment; enthesitis, dactylitis and uveitis; skin and nail involvement; functional situation and quality of life; radiographic evaluation; analytical determinations; treatment; axial and peripheral flare-ups.
ConclusionsThe REAPSER study includes a cohort of patients with recent-onset PsA, before the disease course was modified by disease-modifying antirheumatic drugs prescribed in rheumatology departments. Exhaustive information collected in each visit is expected to be an important data source for future analysis.
Describir la metodología del Registro Español de Artritis Psoriásica de reciente comienzo de la Sociedad Española de Reumatología (REAPSER), así como sus fortalezas y limitaciones. El objetivo principal del proyecto es identificar factores pronósticos de la evolución clínica y radiográfica en una cohorte de pacientes que padecen artritis psoriásica (APs) diagnosticada con menos de 2años de evolución.
Material y métodoEstudio observacional, prospectivo (2años de seguimiento; periodicidad anual de las visitas), multicéntrico. La intención en la visita basal fue reflejar la situación del paciente antes de que la evolución de la enfermedad se viese modificada por los tratamientos pautados en los servicios de reumatología. Los pacientes fueron invitados a participar consecutivamente en una de sus visitas habituales al reumatólogo. El tamaño muestral finalmente alcanzado fue de 211pacientes. Se recogen datos sociodemográficos; de situación laboral; historia familiar; antecedentes personales y comorbilidad; antropométricos; estilo de vida; uso de los servicios de salud; situación clínica al diagnóstico de APs; afectación articular y dolor espinal; dolor y valoración global de la enfermedad; entesitis, dactilitis y uveítis; afectación cutánea y ungueal; situación funcional y calidad de vida; evaluación radiográfica; determinaciones analíticas; tratamiento; brotes en esqueleto axial y periférico.
ConclusionesEl estudio REAPSER incluye una cohorte de pacientes con APs de inicio reciente reclutados antes de que la evolución de la enfermedad se viese modificada por la prescripción de FAME en los servicios de reumatología. Se espera que la información exhaustiva recogida en las visitas suponga una amplia fuente de datos para futuros análisis.
Psoriatic arthritis (PsA) is a chronic inflammatory disease of the joints classified in the spondyloarthritis group. It has been estimated that prevalence in patients with psoriasis is approximately 20%–30%.1,2 The joint phenotype of the disease is highly variable (oligoarthritis, polyarthritis, distal involvement, mutilating and/or spondylytic involvement), and that it may present in different evolutionary combinations over time.
PsA has a considerable impact on physical function and everyday life activities, above that of patients who present with psoriasis.3,4 Also, these patients frequently present with associated extra-articular symptoms and comorbidities, mainly cardiovascular, metabolic syndrome, diabetes, Crohn's disease, ocular pathology (mostly uveitis), non alcoholic fatty liver disease, depression and anxiety.5 The clinical spectrum is diverse and potentially serious for which a multidisciplinary approach is required due to its systemic nature.6
Association has been observed between late diagnosis of PsA and the development of peripheral joint erosion and poorer scores in the HAQ7 questionnaire, together with greater disease progression in patients who are treated after over 2 years of symptom onset evolution.8
However, there are few studies in which prospective follow-up of a cohort of patients with recent onset of PsA has been followed (defined by the onset of symptoms less than 2 years previously) in conditions of regular clinical practice9,10 and no sufficient evidence exists regarding optimum treatment.11
For this reason the Spanish Registry of recent-onset Psoriatic Arthritis was founded by the Spanish Rheumatology Society (REPSAER), the main objective of which was to identify prognostic factors of the clinical and radiographic disease course in a cohort of patients who had suffered from PsA diagnosed within 2 years of symptom evolution. This study describes the project methodology and its possible strengths and limitations.
MethodologyGeneral designMulticentre, longitudinal, observational, prospective study (2 years of follow-up, annual check-ups).
Reference populationPatients with PsA of recent onset (defined as within 2 years of evolution since onset of symptoms attributable to the disease).
Study sample. Selection criteriaInclusion criteria:
- 1.
Adults of both sexes, 18 years of age or older.
- 2.
Compliance of the CASPAR classification criteria.12
- 3.
PsA with a duration of under 2 years since onset of symptoms.
- 4.
Patients attended in rheumatology departments of the centres which participated in the study.
- 5.
Able to effectively communicate with the people conducting the study and to complete the questionnaires themselves.
Exclusion criteria:
- 1.
Patients who were participating in the clinical trial of any product under investigation one month prior to visit 0 or during the study.
- 2.
Very serious or terminal illness.
- 3.
Patients with any physical disability not attributable to PsA or mental patients.
The centres were invited with reference to criteria relating to geographical aspects, services provided in each hospital and the population attended. They were all required to have a dermatologist to assist with data collection. Thirty three centres finally participated, distributed into 21 of the 55 provinces in Spain. The list of participating centres is contained in Appendix A.
Patient recruitmentInitially all participating centres were to recruit the same number of patients, to be fixed beforehand. However, during the course of the study, due to the different recruitment capacity in the different centres, it was decided that each one of them would include patients in accordance with their capacity.
The baseline visit intention was to reflect the patient situation prior to the evolution of the disease being modified by treatments regulated by the rheumatology departments. The patients who participated were therefore not to have been treated for more than 3 weeks with methotrexate, leflunomide or apremilast, and could not be in treatment with biologic DMARDS. These intervals were fixed according to mean time from treatment initiation until the beginning of treatment response being 4weeks in the case of synthetic DMARDS and 1 week in the case of biologic DMARDS. In cases where the patient had been taking synthetic DMARDS for over 3 weeks, we confirmed with the researcher rheumatologist that the patient sill had not responded at the time of the baseline visit; this was exceptional (6 patients), and for all of them the time which passed from synthetic DMARDS initiation was under 2 months.
If a patient with psoriasis in treatment with synthetic or biologic DMARDS developed PsA and was referred to the rheumatology department for diagnosis and management, they could be included in the study. The intention of the baseline visit reflecting the situation of the patient prior to the course of the disease being changed by treatment prescribed by the rheumatology service would be complied with.
The patients were invited to participate consecutively in one of their regular visits to the rheumatologist. Patient access to the rheumatology services were the normal ones of the participating services (basically from primary care and dermatology consultancies). The recruitment period began in November 2014 and terminated in October 2016.
All the patients gave their informed consent. The participating centres assigned an identification code to each of the participants to maintain data confidentiality in accordance with the law in force (RD 1720/2007 which develops the Organic Law 15/1999, of 13th December, on Personal Data protection). The study was approved by the Research Ethics Committees of the participating centres.
Variables and measurement- a)
Socio-demographic data: date of birth: gender; civil status (married/cohabiting, separated/divorced, widowed, single); educational level (no education, primary education, secondary education, university studies).
- b)
Employment status: professional activity, coded in accordance with the National Occupation Classification (CNO2011)13; current employment status (retired/pensioner, unemployed, actively employed, housewife, student); employment disability (without temporary or permanent disability; sick leave during the last year, cause and duration in days; changes of employment due to illness in the last year.
- c)
Family history (father, mother, grandparents, brothers/sisters of: psoriatic arthritis, other inflammatory arthritis, psoriasis, inflammatory intestinal disease.
- d)
Personal history and comorbidity, year of diagnosis, treatments (using review of medical history): Charlson comorbidity index, adjusted by age14; cardiovascular risk factors (hypertension, diabetes mellitus, hyperlipidaemia); cardiovascular events (myocardial infarction, stroke, peripheral vascular disease, ischaemic vascular disease); intestinal inflammatory disease (Crohn's disease, ulcerous colitis or other inflammatory intestinal disease); infectious diseases (tuberculosis, HIV or other infectious diseases); neoplasms and location; fibromyalgia, depression.
- e)
Anthropometric data: weight, height, BMI, waist measurement, hip measurement and waist to hip measurement.
- f)
Lifestyle: tobacco habit (patients who state they have smoked at least 100cigarettes in their life and at time of visit they smoke every day or several days, are classified as “current smoker”. Patients who state they have smoked under 100 cigarettes in their whole life and at the time of visit they do not smoke at all are classified as “ex-smokers”. Patients who state they have never smoked 100 cigarettes are defined as “non smokers”. This classification is the one used in the Health Data and Disability System of the Centres for the Control and Prevention of Diseases (https://www.cdc.gov/nchs/nhis/tobacco/tobacco_recodes.htm). Alcohol consumption (measured in units of standard drink per week and evaluated using the Systematic Interview of Alcohol Consumption).15 Physical activity (assessed with the short form version of the International Physical Activity Questionnaire [IPAQ]).16
- g)
Use of health services in the last year (through review of medical files): hospitalizations (Yes/No) and reason; orthopaedic surgery (Yes/No) and type; number of visits to: primary care, rheumatology, emergency departments, other specialties.
- h)
Clinical situation at diagnosis of PsA: year of presentation of PsA symptoms, date of a PsA diagnosis, origin of patient (primary care, rheumatology, dermatology, others) clinical form (axial, peripheral, mixed) and joint pattern (oligoarticular, polyarticular, distal, mutilant, spondilytical).
- i)
Joint involvement and back pain: number of painful joints (NAD28 and NAD68); number of swollen joints (NAT28 and NAT66); chest expansion, distance between tongue base and wall; modified Schöber test; lateral flexion of spine; intermalleolar distance; finger floor distance, cervical rotation, assessment of the patient of night time pain in the back during the previous week on a scale of 0 (no pain) to 10 (very intense); patient assessment of back pain in general during the last week on a scale of 0 (no pain to 10 (very intense); BASDAI index.17
- j)
Pain and overall assessment of the disease during the last week: evaluation of overall pain provided by the patient on a scale of 0 (no pain) to 10 (very intense); overall evaluation of the disease provided by the patient on a scale of 0 (they feel very well) to 10 (they feel very bad); overall evaluation of the disease provided by the physician on a scale of 0 (level of minimum activity) to 10 (level of maximum activity).
- k)
Enthesitis, dactylitis and uveítis: extended version of the MASES18 index; presence of dactylitis (Yes/No) and number of fingers affected; presence of uveitis, from the previous visit of the study until the current one (Yes/No) and laterality.
- l)
Skin and nail involvement (assessed by a dermatologist): cutaneous psoriasis (Yes/No); year of presentation of the psoriasis; clinical type (psoriasis vulgar [in plaques], in drops, erythrodermic, general pustular, localized pustular, inverted, others); special locations (psoriasis of the scalp, nail bed, palmoplantar, intergluteal fold and/or perianal, palmoplantar pustular, mucous membrane involvement); treatment for psoriasis and year of initiation (topical treatment, phototherapy, retinoids, methotrexate, cyclosporine, etanercept, infliximab, adalimumab, ustekinumab, others). Body surface area (BSA) affected by psoriasis; PASI index19; nail diseases (number of fingers and toes affected in each hand and each foot).
- m)
Functional situation and quality of life: HAQ20 questionnaire, PsAID21 questionnaire, BASFI22 index, SF-3623questionnaire.
- n)
Radiographic assessment: BASRI24,25 index, Steinbrocker method modified for PsA.26
- o)
Lab analysis determinations: ESR, PCR, rheumatoid factor, HLA B27, blood parameters, glucose, uric acid, total proteins, albumin, bilirubin, liver function tests, (GOT, GPT y GGT), total cholesterol, HDL cholesterol, LDL cholesterol, triglycerides.
- p)
PsA treatment, starting date, end date, reason for withdrawal: NSAID, glucocorticoids, synthetic DMARDS (methotrexate, leflunomide, sulfasalazin, apremilast, cyclosporine), biologic DMARDS (adalimumab, etanercept, infliximab, golimumab, ustekinumab, certolizumab, secukinumab). In follow up visits, in the case of DMARDS, it was also noted whether there was therapy compliance (using the question “is the patient complying with treatment?”, with response options of “Yes/no/don’t know”) and for biologic DMARDS the administration guideline was also recorded (standard/optimization regimen).
- q)
Number of PsA outbreaks and date of last outbreak: in axial skeleton (defined as any inflammatory episode affecting the axial skeleton [chest and/or spine-pelvis] assessed as such by a rheumatologist between the previous and current study visit) and in peripheral joints (defined as any inflammatory joint episode, dactylitic or of the observed by a rheumatologist between the previous and present study visit).
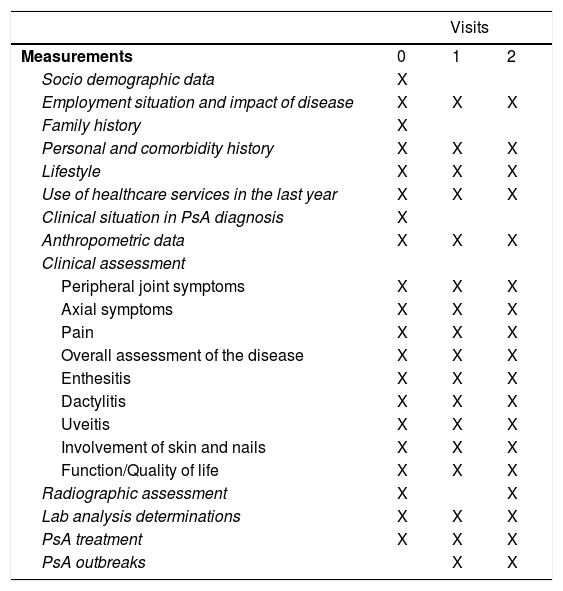
Table 1 lists the measurements made in each study visit. These measurements will allow evaluation to be made of the disease through indexes, such as the Disease Activity for Psoriatic Arthritis (DPSAA)27 or the Psoriatic Arthritis Disease Activity Score (PASDAS).28
Measurements made at each study visit.
| Visits | |||
|---|---|---|---|
| Measurements | 0 | 1 | 2 |
| Socio demographic data | X | ||
| Employment situation and impact of disease | X | X | X |
| Family history | X | ||
| Personal and comorbidity history | X | X | X |
| Lifestyle | X | X | X |
| Use of healthcare services in the last year | X | X | X |
| Clinical situation in PsA diagnosis | X | ||
| Anthropometric data | X | X | X |
| Clinical assessment | |||
| Peripheral joint symptoms | X | X | X |
| Axial symptoms | X | X | X |
| Pain | X | X | X |
| Overall assessment of the disease | X | X | X |
| Enthesitis | X | X | X |
| Dactylitis | X | X | X |
| Uveitis | X | X | X |
| Involvement of skin and nails | X | X | X |
| Function/Quality of life | X | X | X |
| Radiographic assessment | X | X | |
| Lab analysis determinations | X | X | X |
| PsA treatment | X | X | X |
| PsA outbreaks | X | X | |
We initially planned to recruit 295 patients, assuming that there could be up to 25% of losses throughout follow-up. This sample size would make it possible to detect a relative risk of >2.30 as significant, exposure of 50%, confidence interval of 95% and statistical power of 80%.
The final sample size was 211patients.
Data processingData will be monitored online throughout the study, to correct incongruence or data which are missing. Furthermore, 60% of baseline visits will be monitored in situ.
Periodical meetings will be made of researchers with study coordinators, so as to resolve doubts and maintain uniformity of data collection. Whenever in doubt, the researchers may contact the coordinators throughout fieldwork.
DiscussionThe REPSAER study methodology has been described in this study. Members from both the Spondyloarthritis Group of the Spanish Society of Rheumatology (GRESSER) and the Psoriatic Arthritis Group of the SER GEPSAOSER) participated in this study and is the only multicentre cohort of patients with PsA has recently begun in Spain up until now.
On an international level, there is little data on prognostic and predictive factors of recent-onset PsA management in clinical practice.29–31 In the literature publications of the Swedish cohort of patients with early onset PsA (SwePsA) stand out. This began in 1999 and data from 6 rheumatology services from different cities in Spain were recorded. Like the REPSAER, all the patients fulfilled the CASPAR criteria, which have been shown to be valid for early stage diagnoses.32 The latest published articles, with a 5-year follow-up data include almost 200 patients.30,31 These are patients with under 2 years of PsA symptom onset when they became part of the study. However, 15% were already receiving treatment with DMARDS in the inclusion visit and 13.2% of the total presented with minimum disease activity in that visit (according to the Coates et al.33 definition established with participation from experts belonging to the Group for Research Assessment of Psoriasis and Psoriatic Arthritis [GRAPPA]).
In the REPSAER the inclusion moment sought was to be as homogenous as possible for all patients, so as to increase study validity. To this end, although the initial intention was recruitment exclusively at the time of PsA diagnosis in the participating rheumatology services, due to the complexity this entailed we chose to extend the time window, with an essential condition being that at the baseline visit the course of the disease had not been modified by treatment with DMARDS prescribed from PsA diagnosis in the rheumatology departments. In all cases the time of PsA symptom onset had to be under 2 years. The difficulty in recruitment made it necessary to extend the initial inclusion period (which was one year) and this made it impossible to obtain the prefixed sample size (295 patients). However, this number was calculated with several assumptions regarding outcome occurrence during the follow-up which maximized the necessary sample size. The 211 patients who were finally recruited would mean a statistically significant RR≥2.3 if the non exposed outcome was 11%; if there were a 25% of follow-up losses, significant RR would be detected as≥2.6.
Another key strength of the study was the exhaustive information collected during the visits, regarding socio-demographic data, life habits and functional ability, together with clinical, radiological, blood and treatment parameters. This should enable REPSAER to become an important source of data for future analysis and study.
With regards to study limitations, the reduction in the sample size could lower the ability to detect significant associations and reduce the percentage of losses during follow-up which would be considered acceptable. Furthermore, the unequal distribution in the number of patients recruited in each centre could affect the geographical representation of the study for the whole of Spain. This cohort does not include patients from all of the autonomous communities. Specifically, there are no data on centres in Aragón, Cantabria, Castilla-La Mancha, Extremadura, La Rioja or Navarre.
ConclusionsThe REPSAER study includes a cohort of patients with PsA of recent onset recruited prior to the evolution of the disease being altered by the prescription of DMARDS in rheumatology services. It is hoped that the exhaustive information collected in the visits will be a broad source of data for future analysis and research.
FinancingREPSAER is financed by Abbvie. Abbvie did not intervene in the study design, data collection, analysis or in the writing of this article.
Conflict of interestsThe authors have no conflict of interests to declare relating to the content of this document.
Our thanks to Dr. José Luis Fernández Sueiro, responsible for the initial conception and development of this study. Also to Carlos Manuel Tilve Álvarez, for IT support in the electronic platform of the study.
The following are the supplementary data to this article:
The names of the components of the REAPSER Project Working Group are listed in Appendix A.
Please cite this article as: Queiro R, Laiz A, Seoane-Mato D, Galindez Agirregoikoa E, Montilla C, Park HS, et al. Registro Español de Artritis Psoriásica de Reciente Comienzo (estudio REAPSER). Objetivos y metodología. Reumatol Clin. 2019;15:252–257.
- Spontaneous pneumomediastinum: An extra muscular manifestation of anti-MDA5 dermatomyositis. Report of 2 cases
- The impact of COVID-19 and other factors on the usage status of the biologic drug therapies for rheumatoid arthritis: A study from Vietnam
- Analysis of factors involved in the development of humoral response to vaccination against SARS-CoV-2 in patients with rheumatic pathology under biological treatment
- The “autoimmune/inflammatory syndrome induced by adjuvants” (ASIA) after COVID-19 infection: A case report
articles


