

To estimate the annual cost of temporary work disability (TWD) caused by musculoskeletal diseases (MDs) in Spain and its variations between regions (autonomous communities: ACs) and paying institutions.
MethodDescriptive study of the costs of MD-related TWD in ACs in 2007. The Spanish National Institute of Social Security (NISS) provided aggregate data. Extrapolations to the rest of the TWD payers (mutual societies and employers) were used.
ResultsMDs were the leading cause of TWD in Spain in 2007, causing 908781 episodes of TWD (18% of the total), 39342857 lost working days (23%), and a cost of 1702 million euros (23%). The annual incidence of TWD episodes per 1000 employed was 45. The cost per TWD process was 1873 €, ranging from 1391 € (La Rioja) to 2429 € (The Basque Country).
ConclusionMDs produce annually in Spain over 39 million days lost by TWD with a cost of over 1700 million euros. Regions observed wide variations of the TWD cost.
Estimar el coste anual de la incapacidad temporal (IT) ocasionada por las enfermedades musculoesqueléticas (EME) en España y su variabilidad entre comunidades autónomas (CC. AA.) y entidades pagadoras.
MétodoEstudio descriptivo de costes por IT debida a EME en las CC. AA. en el 2007. Se utilizaron datos agregados del Instituto Nacional de Seguridad Social (INSS) y extrapolaciones a las entidades que realizan el pago de la IT (INSS, mutuas y empresas).
ResultadosLas EME fueron la primera causa de IT en España en 2007, produciendo 908.781 episodios de IT (18% del total), 39.342.857 días de baja (23%) y 1.702 millones de euros de coste (23%). La incidencia anual de procesos de IT por EME por cada 1.000 personas ocupadas fue de 45. El coste por proceso de IT fue de 1.873 oscilando entre un mínimo de 1.391 € (La Rioja) y un máximo de 2.429 € (País Vasco).
ConclusiónLas EME producen anualmente en España más de 39 millones de días de baja por IT, con un coste superior a 1.700 millones de euros. El coste de la IT tiene una amplia variabilidad entre CC. AA.
Musculoskeletal diseases (MDs) are the leading cause of disability worldwide1 and have a high impact on the direct (medical) and indirect (sick leave) costs. Sick leaves in Spain, where they are temporary, are known as temporary disability (TD). The economic benefit of TD is a percentage of the base salary, which mainly depends on the amount. The payment of the benefit, from day 16, is responsibility of the National Social Security Institute (INSS), or a mutual agreement, as a partner in the management company2 being paid by the employer from payment day 4 to 15. The provision for days 1–3 depends on the type of affiliation and labor agreements. TD process starts and ends at the primary care physician level.
Although there are some studies,3,4 no information was found on the cost of TD due to MD or its variability by Region (CC. AA.) or payer. For this reason, we decided to perform this study aimed at estimating the annual cost of TD caused by MD in Spain and its variability between CC. AA. and payers.
MethodologyThis was a descriptive study of cost estimation of TD caused by MD in Spain, using secondary data from INSS. The INSS provided a table for each Spanish province which consisted the number of TD processes, the number of total days of TD and the mean duration of the process, by sex and age of TD processes regarding common diseases in 2007. The INSS classifies a process as MD parting from an official evaluation as part of ICD-9-CM coding. In the absence of data on TD due to MD, the number of processes and their duration were estimated as the ratios of affiliation, incidence and duration in each other with respect to INSS5. To estimate costs, we considered the amount of the benefit and the days of TD paid by the INSS or mutual.2,6,7
The additional part paid for by the employer varies with the type of collective agreement. Given the variability of the agreements, it was assumed that, on average, companies pay 80% of the employee's salary the first 3 days, completing what is paid for by the INSS or mutual to 80% from day 4 to 20, and even 90% from day 21 onwards. To estimate the costs by type of affiliation, we considered the proportion of workers belonging to each regime: General Regime (RG), Special Scheme for Self-Employed (RETA), Special Agricultural Self-paid Scheme, Special Agricultural Scheme paid by the employer, Home makers regime (REEH), Special Scheme for Coal Mining (REMC) and Special Scheme for Sea workers.8 The average daily INSS contribution base for the affiliate scheme was adjusted for changes in salary by gender and CC. AA.9 Information on employed persons and GDP and for the CC. AA. was obtained from the National Statistics Institute.9–11
ResultsMDs were the leading cause of TD in Spain, producing 908781 TD processes (18% of all processes), 39342857 lost work days (23% of days lost per TD) and a cost of 1702 million euros (23% of the cost of all TD l). TD processes of longer duration were caused by mental illness, which accounted for 11% of TD costs.
The average cost of an episode of TD due to MD was 1873 €. In all, 57% of the processes and 53% of the cost of TD due to MD occurred in women. However, the average cost of TD was lower in women than in men: 1746 € vs 2040 €.
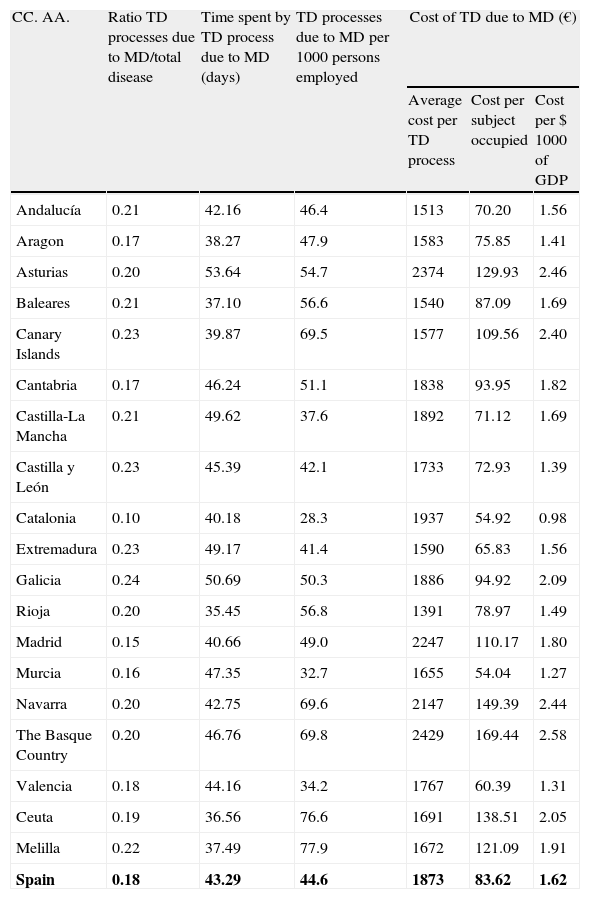
Of the TD processes, 18% is caused by MD, but in Galicia this was 24%, while in Catalonia it was 10%. The average duration of an absence due to MD in Spain is 43 days, but varies between a maximum of 54 days in Asturias and a minimum of 35 days in La Rioja. The annual number of TD processes due to MD per 1000 employed persons was 44.6 in Spain, ranging from a high of 70 in the Basque Country, Navarra and Canarias (except Ceuta and Melilla) to a minimum of 28 in Catalonia. The mean cost of a TD process due to MD in Spain was 1873 €, with a maximum value in the Basque Country (2429 €) and a minimum in La Rioja (1391 €) (Table 1).
Temporal Disability and Costs Caused by MD per CC. AA. (2007).
| CC. AA. | Ratio TD processes due to MD/total disease | Time spent by TD process due to MD (days) | TD processes due to MD per 1000 persons employed | Cost of TD due to MD (€) | ||
| Average cost per TD process | Cost per subject occupied | Cost per $ 1000 of GDP | ||||
| Andalucía | 0.21 | 42.16 | 46.4 | 1513 | 70.20 | 1.56 |
| Aragon | 0.17 | 38.27 | 47.9 | 1583 | 75.85 | 1.41 |
| Asturias | 0.20 | 53.64 | 54.7 | 2374 | 129.93 | 2.46 |
| Baleares | 0.21 | 37.10 | 56.6 | 1540 | 87.09 | 1.69 |
| Canary Islands | 0.23 | 39.87 | 69.5 | 1577 | 109.56 | 2.40 |
| Cantabria | 0.17 | 46.24 | 51.1 | 1838 | 93.95 | 1.82 |
| Castilla-La Mancha | 0.21 | 49.62 | 37.6 | 1892 | 71.12 | 1.69 |
| Castilla y León | 0.23 | 45.39 | 42.1 | 1733 | 72.93 | 1.39 |
| Catalonia | 0.10 | 40.18 | 28.3 | 1937 | 54.92 | 0.98 |
| Extremadura | 0.23 | 49.17 | 41.4 | 1590 | 65.83 | 1.56 |
| Galicia | 0.24 | 50.69 | 50.3 | 1886 | 94.92 | 2.09 |
| Rioja | 0.20 | 35.45 | 56.8 | 1391 | 78.97 | 1.49 |
| Madrid | 0.15 | 40.66 | 49.0 | 2247 | 110.17 | 1.80 |
| Murcia | 0.16 | 47.35 | 32.7 | 1655 | 54.04 | 1.27 |
| Navarra | 0.20 | 42.75 | 69.6 | 2147 | 149.39 | 2.44 |
| The Basque Country | 0.20 | 46.76 | 69.8 | 2429 | 169.44 | 2.58 |
| Valencia | 0.18 | 44.16 | 34.2 | 1767 | 60.39 | 1.31 |
| Ceuta | 0.19 | 36.56 | 76.6 | 1691 | 138.51 | 2.05 |
| Melilla | 0.22 | 37.49 | 77.9 | 1672 | 121.09 | 1.91 |
| Spain | 0.18 | 43.29 | 44.6 | 1873 | 83.62 | 1.62 |
CC. AA., autonomous community; MD, musculoskeletal disease; TD, temporary disability; GDP, gross domestic product.
In bold the average for Spain is represented.
The average cost per TD due to MD per employed person in Spain was 83.6 €; the Basque Country had the highest (169 €), while Murcia (54 €) had the lowest cost per employee. The cost of TD due to MD in Spain represented 1.62 € per 1000 € of GDP. The Basque Country (2.58 €) had the highest TD costs due to MD per 1000 € of GDP and Catalonia (0.98 €), the lowest (Table 1).
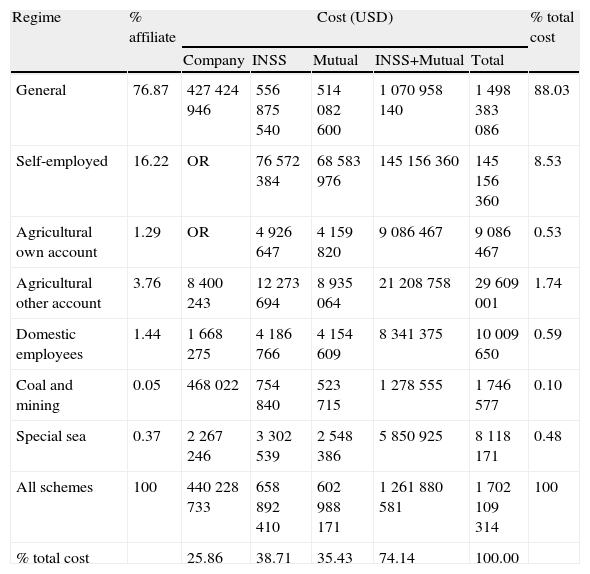
Schemes with a higher proportion of unionized workers are the RG (76.87%) and RETA (16.22%), and consequently are schemes in which the higher costs occur in absolute terms: 88% (1 .498 million) of costs occurred in the RG members, followed by those from RETA (8.5% of costs). Members of the REMC had the lowest absolute cost, but a higher cost per member (0.10% of costs and 0.05% of members). In all, 39% of the costs are borne by the INSS, 35% from mutual and 26% is paid by companies (Table 2).
Cost of TD Due to MD Per System and Payer in Spain in 2007.
| Regime | % affiliate | Cost (USD) | % total cost | ||||
| Company | INSS | Mutual | INSS+Mutual | Total | |||
| General | 76.87 | 427424946 | 556875540 | 514082600 | 1070958140 | 1498383086 | 88.03 |
| Self-employed | 16.22 | OR | 76572384 | 68583976 | 145156360 | 145156360 | 8.53 |
| Agricultural own account | 1.29 | OR | 4926647 | 4159820 | 9086467 | 9086467 | 0.53 |
| Agricultural other account | 3.76 | 8400243 | 12273694 | 8935064 | 21208758 | 29609001 | 1.74 |
| Domestic employees | 1.44 | 1668275 | 4186766 | 4154609 | 8341375 | 10009650 | 0.59 |
| Coal and mining | 0.05 | 468022 | 754840 | 523715 | 1278555 | 1746577 | 0.10 |
| Special sea | 0.37 | 2267246 | 3302539 | 2548386 | 5850925 | 8118171 | 0.48 |
| All schemes | 100 | 440228733 | 658892410 | 602988171 | 1261880581 | 1702109314 | 100 |
| % total cost | 25.86 | 38.71 | 35.43 | 74.14 | 100.00 | ||
MDs were the leading cause of TD in Spain in 2007, representing 18% of processes, 23% of days lost and 23% of the cost of TD caused by all diseases. The mean duration per TD process due to MD is approximately one and one-half months (43 days). The proportion of TD processes due to MD in Spain was higher in women than in men, consistent with the fact that the MDs are more common in women.12 However, the average cost per episode for TD was lower in women than in men, perhaps due to the different distributions of the type of employment and wages between the genders.
The observed variability in the number of processes, duration and costs between CC. AA. is consistent with previous studies.3,4 However, in our study the proportion of TD due to MD in Catalonia (10%) was lower than that of a 2009 study, where MDs were the second cause of TD (19% of total).13 One possible explanation for this difference could be the improvement in diagnostic coding in Catalonia, as in the Catalonia INSS data for 2007, 42% of TD processes were not diagnosed.
Variability in TD length between CC. AA.14 had been previously explored, referring to the factors influencing return to work after TD, which were the CC. AA., age, gender and economic activity of the patient. It is difficult to find an explanation for the differences in the number of TD processes due to MD between CC. AA. after adjusting for the employed population. They could be due to structural factors, for example, the different compositions of the working population, but could also be due to organizational aspects, such as differences in the control of sick leave between CC. AA. factors.
The cost per procedure varies widely depending on the type of affiliation. For example, the average cost of a TD process due to MD in REMC is 3776, twice the average and 5 times higher than that in REEH. This is due, among other reasons, to the fact that the average contribution base of REMC is much higher than in REEH (82.86 € vs 22.18 €). According to the affiliate scheme and the entity that pays the TD, the INSS (39%) and mutual (35%) bear most of the cost of TD due to MD, and the employer (26%) comes in third. Payment for TD is a little lower in mutual (35% vs INSS 39%), because, although for each worker covered by the INSS there are 1.35 covered by mutual, prevalence and the duration of TD processes are 20% lower in mutual compared to that in INSS.5
One limitation of the study is that the information relates to the year 2007 and the findings must be interpreted in the context of the economic situation and the Spanish health system at that date. Another limitation could be that the data provided by the INSS may have a misclassification bias, since the data come from the “official reports” given by doctors, who might assign the process of TD to a given condition when a patient has more than one. This and other potential limitations of the study come primarily from the limited information available for research. Consequently, it is crucial to improve information systems and research projects that contribute to produce knowledge on the indirect costs of disease in Spain.
In conclusion, MDs were the leading cause of TD in Spain in 2007, producing more than 900000 episodes of TD, 39 million days off work and a considerable cost to the INSS, and mutual companies, which together amounted to 1700000000 euros. There is a wide variability in CC. AA. on different indicators analyzed and membership schemes.
This article is an abridged version of the “Cost of temporary disability due to musculoskeletal diseases in Spain” report. This report can be obtained at http://www.taiss.com/publi/absful/informe-coste-incapacidad-temporal-enfermedades-musculo-esqueleticas-taiss.pdf.
Ethical ResponsibilitiesProtection of people and animalsThe authors declare that no experiments have been performed on humans or animals.
Data confidentialityThe authors state that no patient data appear in this article.
Right to privacy and informed consentThe authors state that no patient data appear in this article.
FundingThis study was funded by the Abbott Foundation, which was not involved in the analysis or in drafting the manuscript.
Conflicts of InterestThe authors declare no conflicts of interest.
We appreciate the valuable collaboration of the INSS for the information provided, for their advice and for their dedication to this work. We also thank Asepeyo, for information used to verify the consistency of our assumptions regarding the mutual.
Please cite this article as: Lázaro P, Parody E, García-Vicuña R, Gabriele G, Jover JÁ, Sevilla J. Coste de la incapacidad temporal debida a enfermedades musculoesqueléticas en España. Reumatol Clin. 2014;10:109–112.


