


We want to know if the ultrasound examination of the Achilles tendon in spondyloarthritis is different compared to other rheumatic diseases.
Materials and methodsWe studied 97 patients divided into five groups: rheumatoid arthritis, spondyloarthritis, gout, chondrocalcinosis and osteoarthritis, exploring six elementary lesions in 194 Achilles entheses examined.
ResultsIn our study the total index ultrasonographic Achilles is higher in spondyloarthritis with significant differences. The worst elementary spondyloarthritis lesions for discriminations against other pathologies were calcification.
ConclusionsThis study aims to demonstrate the discriminant validity of Achilles enthesitis observed by ultrasound in spondyloarthritis compared with other rheumatic diseases that may also have ultrasound abnormalities such enthesis level.
Analizar si la exploración ecográfica del tendón de Aquiles es diferente en las espondiloartritis respecto de otras enfermedades reumáticas.
Material y métodosSe estudia a 97 pacientes divididos en 5 grupos: artritis reumatoide, espondiloartritis, gota, condrocalcinosis y artrosis, explorándose 6 lesiones elementales en las 194 entesis de Aquiles examinadas.
ResultadosEn nuestro estudio, el índice total ecográfico en tendón de Aquiles es mayor en el grupo de espondiloartritis con diferencias significativas. La lesión elemental que peor discrimina las espondilitis respecto de otras patologías es la presencia de calcificaciones.
ConclusionesEste estudio pretende demostrar la validez discriminante de la entesitis aquílea observada por ecografía en las espondiloartritis en comparación con otras enfermedades reumatológicas que también pueden presentar alteraciones ecográficas a nivel de dicha entesis.
Enthesitis is the most characteristic condition in spondyloarthritides (SpA). In their article, “The enthesis organ concept and its relevance to the spondyloarthropathies”,1 Michael Benjamin and Dennis McGonagle propose this concept and use it to explain their understanding of this “organ”. It is thought to have a biomechanical basis that, in a context of genetic predisposition, triggers an autoinflammatory process that causes the disease affecting the entheseal fibrocartilage.2–4 The enthesis organ concept provides an explanation for the connection among bursitis, synovitis and enthesitis.5,6 The Achilles tendon has been considered an example of an enthesis organ.
On the other hand, ultrasound is a highly valuable tool in the diagnosis and assessment of the activity of inflammatory diseases. Several studies have validated ultrasound for the evaluation of entheses.
The ultrasound index of Balint et al. (the Glasgow Ultrasound Enthesitis Scoring System [GUESS])7 rates the Achilles tendon, plantar tendon, distal and proximal patellar ligaments and quadriceps tendon. The Sonographic Enthesitic Index of Alcalde et al.8 examines the same entheses, but distinguishes between acute and chronic lesions. D‘Agostino et al.9,10 introduced Doppler imaging to assess activity. Hamdi et al.11 correlated the Maastricht Ankylosing Spondylitis Enthesitis Score (MASES for ultrasound) and a Doppler score with the visual analog scale (VAS) for pain, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), the Bath Ankylosing Spondylitis Functional Index (BASFI), and the Ankylosing Spondylitis Quality of Life (ASQoL) instrument. Chronic ultrasound lesions did not correlate with any parameter.
In their study, De Miguel et al.12,13 used the Madrid Sonography Enthesitis Index (MASEI) to explore 6 entheses (the 5 mentioned above and a triceps tendon) and 6 variables (including Doppler signal) associated with the elementary lesions. They reported a sensitivity of 83.3% and a specificity of 82.8%. This may be the most sensitive method for evaluating inflammatory lesions and structural damage.
Evaluation of the discriminant validity of enthesis ultrasound has been limited to studies involving mechanical processes, healthy processes and SpA14 and, in some cases, rheumatoid arthritis (RA) (De Miguel et al.13; D’Agostino et al.9). However, until now, it has not been studied in other enthesopathies, like the microcrystalline diseases, which also affect the entheses.
Thus, the main objective of this study is to compare the discriminant validity of enthesis ultrasound in different models of rheumatic diseases.
On the other hand, the assessment of several entheses is too time-consuming to be easily carried out in routine practice; therefore, to improve the feasibility of this study of the discriminant power of ultrasound, we have focused on the Achilles enthesis, as it is the most representative example of these structures.
Materials and MethodsWe performed a cross-sectional, observational, analytical study consisting of 5 arms. The study population was formed by the systematic consecutive recruitment of the first 3 patients to come to a hospital rheumatology department for examination of the lesions to be studied between September and November 2012, provided they consented to being enrolled. They were paired by sex and age. The study was approved by the hospital ethics committees. In addition to demographic data and the Disease Activity Score in 28 Joints (DAS28) for each patient, we recorded the BASDAI and VAS corresponding to the entheses examined.
Each patient underwent ultrasound of the Achilles tendon. The sonographer was blinded to the patient's clinical and diagnostic data. Ninety-seven patients (194 Achilles tendons) were examined and, according to the criteria they met for each disease, were included in 1 of 5 groups: AR (n=20), SpA (n=21), gout (n=17), chondrocalcinosis (CC; n=15) and osteoarthritis (OA; n=24).
Ultrasound ExaminationThe activity and structural damage were assessed by means of the ultrasound examination of 6 elementary lesions of the Achilles tendon. For this purpose, the sonographer underwent training in enthesis ultrasound and a rotation in the unit in which the MASEI had been created, achieving a good overall reliability, according to the kappa statistic and intraclass correlation coefficient.
The findings were scored according to the MASEI for the assessment of the elementary lesions:
- –
Calcifications: none=0; <5mm=1; 5–10mm=2, and ossification >10mm=3.
- –
Structure and thickness were scored as 0 when absent and 1 when present.
- –
Bursa: present (>2mm)=1 and absent (<2mm)=0.
- –
Erosions and Doppler signal: absent=0 and present=3.
We used a Logiq 5 ultrasound system from General Electric Healthcare, with a 12-MHz linear probe for gray scale images and a 6.6-MHz probe for power Doppler, with a 29-dB gain and a pulse repetition frequency of 0.4kHz.
Statistical AnalysisAnalysis of variance (ANOVA) was performed to compare the ultrasound findings in the different subgroups. The values are expressed as the mean±standard deviation.
For the quantitative comparison between SpA and the other diseases, we used Student's t test for independent samples.
ResultsDemographic DataOf the 97 patients, 49 were men (50.51%) and 48, women (49.48%) (Table 1). The mean age was 55.1±9.94 years. There were age-related differences in the numbers of patients with gout, CC and OA, as these diseases develop in older patients.
Variables Corresponding to Each Study Group.
| Achilles tendons (n) | Age (years) | Men (n) | Women (n) | Tendon VAS (0–10cm) | Ultrasound index (0–12) | |
|---|---|---|---|---|---|---|
| Rheumatoid arthritis | 40 | 53.05 | 10 | 10 | 1.55 | 6.75 |
| Spondyloarthritis | 42 | 50.02 | 10 | 11 | 2.28 | 9.61 |
| Gout | 34 | 60.23 | 8 | 9 | 2 | 8.82 |
| Chondrocalcinosis | 30 | 59.8 | 8 | 7 | 0.8 | 5.2 |
| Osteoarthritis | 48 | 54.74 | 13 | 11 | 0.58 | 3.92 |
VAS, visual analog scale.
The mean DAS28 was 3.3 in patients with RA and the BASDAI was 2.93 in those with SpA. The mean VAS score for the entheses was 1.4/10, being ≥2 in the patients with SpA and gout, 1.55 in those with RA and <1 in those with OA and CC.
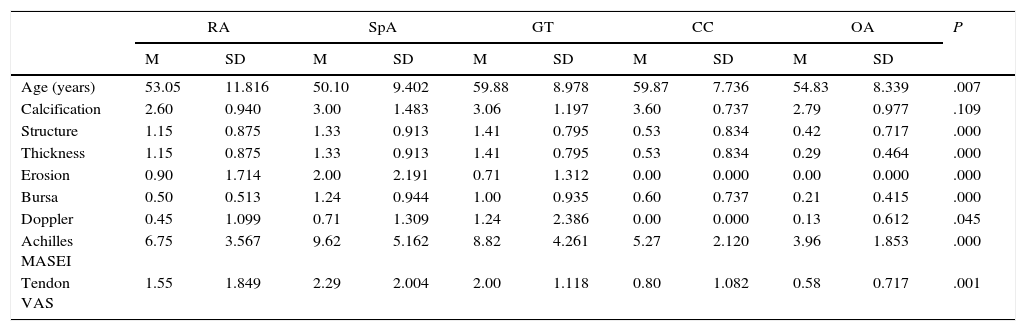
Ultrasound FindingsThe highest score on the ultrasound index corresponded to SpA and the lowest to OA. Table 2 shows the scores for the different elementary lesions.
Comparison Among the Study Groups.
| RA | SpA | GT | CC | OA | P | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | M | SD | ||
| Age (years) | 53.05 | 11.816 | 50.10 | 9.402 | 59.88 | 8.978 | 59.87 | 7.736 | 54.83 | 8.339 | .007 |
| Calcification | 2.60 | 0.940 | 3.00 | 1.483 | 3.06 | 1.197 | 3.60 | 0.737 | 2.79 | 0.977 | .109 |
| Structure | 1.15 | 0.875 | 1.33 | 0.913 | 1.41 | 0.795 | 0.53 | 0.834 | 0.42 | 0.717 | .000 |
| Thickness | 1.15 | 0.875 | 1.33 | 0.913 | 1.41 | 0.795 | 0.53 | 0.834 | 0.29 | 0.464 | .000 |
| Erosion | 0.90 | 1.714 | 2.00 | 2.191 | 0.71 | 1.312 | 0.00 | 0.000 | 0.00 | 0.000 | .000 |
| Bursa | 0.50 | 0.513 | 1.24 | 0.944 | 1.00 | 0.935 | 0.60 | 0.737 | 0.21 | 0.415 | .000 |
| Doppler | 0.45 | 1.099 | 0.71 | 1.309 | 1.24 | 2.386 | 0.00 | 0.000 | 0.13 | 0.612 | .045 |
| Achilles MASEI | 6.75 | 3.567 | 9.62 | 5.162 | 8.82 | 4.261 | 5.27 | 2.120 | 3.96 | 1.853 | .000 |
| Tendon VAS | 1.55 | 1.849 | 2.29 | 2.004 | 2.00 | 1.118 | 0.80 | 1.082 | 0.58 | 0.717 | .001 |
CC, chondrocalcinosis; GT, gout; M, mean; MASEI, Madrid Sonography Enthesitis Index; OA, osteoarthritis; RA, rheumatoid arthritis; SD, standard deviation; SpA, spondyloarthritis; VAS, visual analog scale.
The data are expressed as the mean±standard deviation.
The findings in SpA were compared with those recorded for each of the other 4 groups (Table 2).
- 1.
Spondyloarthritis vs RA: The overall ultrasound values and the value for retrocalcaneal bursitis were significantly higher in SpA. There were no significant differences in calcifications, structure, thickness or Doppler signal. The difference in the values for erosions nearly reached statistical significance.
- 2.
Spondyloarthritis vs gout: The only significant difference was recorded for erosions, which were more common in SpA.
- 3.
Spondyloarthritis vs CC: The values for structure, thickness, erosions, bursitis and Doppler signal were significantly higher in SpA, as was the overall ultrasound score. The value for calcifications was higher in CC, although the difference did not reach statistical significance.
- 4.
Spondyloarthritis vs OA: The values were significantly higher in SpA, with the exception of calcifications.
Until now, there had been no real discriminant validity studies of enthesis ultrasound; the studies had been limited to isolated reports involving healthy individuals or inflammatory diseases like RA.9,13,14 However, the entheses are frequently affected in microcrystalline diseases and in long-standing OA. In this respect, our study is original as it demonstrates, for the first time, the power of certain elementary lesions to discriminate among different diseases, and especially that of the MASEI score for Achilles enthesis, as compared to different models of rheumatic disease (autoimmune, degenerative and microcrystalline); this index only lacks discriminant validity in the evaluation of gout, although the score is also lower in the latter case.
We find it interesting that calcifications in the enthesis have no discriminant value, and that they are even slightly more intense in microcrystalline diseases. The presence of a Doppler signal was greater in SpA, but the difference was significant only with respect to CC and OA. Erosions are the most specific lesions for the diagnosis of SpA, showing significant differences with respect to all of the other diseases studied, with the exception of RA. On the other hand, retrocalcaneal bursitis was also more common in SpA, significantly more so than in RA, CC and OA.
A limitation to the study is the more advanced age of patients with microcrystalline diseases (gout and CC), a bias that is difficult to correct because these diseases develop at later ages. However, if this bias were to exist, it would be reflected in a greater frequency of calcific lesions, which would increase their overall incidence and, thus, their power as discriminating factors with respect to SpA. Thus, we consider that the discriminant validity is maintained. On the other hand, the inclusion of only elderly patients with inflammatory diseases would create a selection bias that would reduce the validity of the study, since the differential diagnosis is most important in the initial phases. Another limitation is the failure to carry out a collective study of the images or assess inter-reader agreement, although the criteria and measurements were standardized in the training received by the sonographers.
In conclusion, we present the first study using ultrasound in an enthesis to assess its value in discriminating among different diseases. We found that the incidences of some lesions, such as erosions and bursae, and the presence of Doppler signals differ significantly depending on the underlying disease. The MASEI in Achilles tendon shows a potential ability to differentiate between SpA and the other diseases studied, with the exception of gout. These findings should lead to further studies to confirm the discriminatory power of enthesis ultrasound.
Ethical DisclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of InterestThe authors declare they have no conflicts of interest.
We wish to thank the members of the nursing staff of the rheumatology department for their help and our patients for their generous collaboration in the study.
Please cite this article as: Expósito Molinero MR, de Miguel Mendieta E. Estudio sobre la validez discriminante de la ecografía de entesis aquílea. Reumatol Clin. 2016;12:206–209.


