

Humor has been described as an effective coping strategy for dealing with chronic pain conditions; likewise, coping strategies predict some clinical outcomes after cognitive-behavioral therapy and mindfulness-based interventions. The present study aims to preliminarily explore the role of humor styles in predicting clinical changes after the multicomponent intervention (MINDSET) that combines mindfulness and psychoeducation for fibromyalgia (FM) patients.
Material and methodsA subsample of 35 patients with FM of the EUDAIMON study, a randomized controlled trial, was used for the present study; linear regressions and Spearman's correlations were computed.
ResultsAffiliative humor and positive/negative ratio humor styles had a unique predictive effect on self-reported clinical changes. Significant correlations between humor styles with functional impact and mindfulness facets were observed.
ConclusionsSome humor styles may imply a better disposition in patients to learn and implement the concepts and resources that the intervention offered.
El humor se considera una estrategia de afrontamiento efectiva para afrontar enfermedades crónicas; asimismo, las estrategias de afrontamiento pueden predecir cambios clínicos experimentados tras intervenciones cognitivo-conductuales y basadas en mindfulness. El presente estudio explora el rol de los estilos de humor en la predicción de cambios clínicos tras una intervención multicomponente (MINDSET, mindfulness+psicoeducación) para pacientes con fibromialgia.
Materiales y métodosEn este estudio participaron 35 pacientes con fibromialgia, una submuestra del ensayo controlado y aleatorizado del estudio EUDAIMON. Se realizaron regresiones lineales y correlaciones de Spearman.
ResultadosEl humor afiliativo y la ratio de estilos positivos/negativos mostraron un efecto predictor en cambios clínicos auto-reportados. Se observaron correlaciones significativas entre estilos de humor, impacto funcional y facetas de mindfulness.
ConclusionesAlgunos estilos de humor pueden implicar una mejor predisposición en los pacientes para aprender y aplicar los recursos que la intervención ofrece.
Fibromyalgia (FM) is a disabling syndrome characterized by chronic widespread pain along with fatigue, stiffness, sleep problems, psychological distress and cognitive disturbances.1
The importance of emotion regulation strategies to face chronic pain has been highlighted in previous studies as they are related to symptomatology and impact of the disease.2 Humor has been considered an effective coping strategy; the humor styles described by Martin, Puhlik-Doris, Larsen, Gray, and Weir,3 which are divided into positive (affiliative and self-enhancing) and negative (self-defeating and aggressive), have been observed to correlate significantly and in the expected direction with self-esteem, positive emotions, optimism, hostility, and psychological distress, among other variables in patients with different pathologies. In chronic pain conditions, there is promising evidence that humor may help in dealing with its related emotional distress.4 In the case of FM, some studies have found that the use of humor was associated with reduced anxiety, psychological distress, and symptoms, and with increased ability to control pain and positive reappraisal.5
Humor has been described as similar to the decentering construct,6 which is the ability to “step back” mentally from a situation to become more fully aware of it, as well as finding alternate ways of interpreting and responding effectively to a given situation. In this regard, some styles of humor may enhance a more flexible psychological response; it is said, a change in perspective to not become fused with mental contents (e.g. negative thoughts) which may enable a more regulated emotional response. Coherently, positive correlations between positive humor styles and mindfulness trait has been previously reported,7 and both coping and mindfulness variables have been found to be moderators of the clinical response to different psychotherapies, including mindfulness-based interventions.8 Mindfulness facets have been observed to be significantly related to FM impact, with higher impact being associated with lower mindfulness levels except for Observing facet, which was positively related; this association suggests that, in FM, this mindfulness facet would be more related to pain amplification rather than mindful observation.9
The present pilot study aimed to examine the predictive effect of humor styles on perceived clinical changes and functional impact after the multicomponent intervention named MINDSET (MINDfulneSs and EducaTion) in a sample of FM patients. In addition, the study explored for the first time the association between humor styles, mindfulness, and the functional impact of FM.
MethodsThirty-five patients from the EUDAIMON project (see Feliu-Soler et al., 2016 for the study protocol)10 participated in the current study, which was performed following the ethical standards laid down in the 1964 Declaration of Helsinki and its subsequent updates. The EUDAIMON project was approved by the Ethics Committee at the Sant Joan de Déu Foundation (PIC-102-15) and all patients signed the informed consent. These patients were offered to participate in the present study as a compensation for being allocated to the passive control arm (usual care) in EUDAIMON. All the participants in this study presented FM according to the American College of Rheumatology 1990 criteria.
The Spanish-validated version of the following questionnaires was administered during the study, next to a socio-demographic questionnaire:
- -
Humor Styles Questionnaire (HSQ).3 It is a 32-item questionnaire that assesses the individual's tendency to experience or use four different humor styles: affiliative, self-enhancing, self-defeating, and aggressive. This questionnaire was administered before the intervention.
- -
The 15-item version of the Five-Facets Mindfulness Questionnaire (FFMQ-15).11 This is a short version of the original FFMQ (with 39 items) that evaluates five facets of mindfulness: Observing, Describing, Acting with awareness, Non-judging and Non-reacting. This questionnaire was administered before the intervention.
- -
Patient Global Impression of Change (PGIC).12 It is a brief scale (6 items) that assesses the individual's perceived global change and the specific improvement in different areas: physical and social functioning, work-related activities, mood and pain. This questionnaire was administered after the intervention.
- -
Revised Fibromyalgia Impact Questionnaire (FIQR).13 This is considered the “gold standard” for assessing functional impact in FM patients; it consists of 21 items that evaluate three domains: physical dysfunction, overall impact, and symptomatology. The FIQR was administered both before and after the intervention.
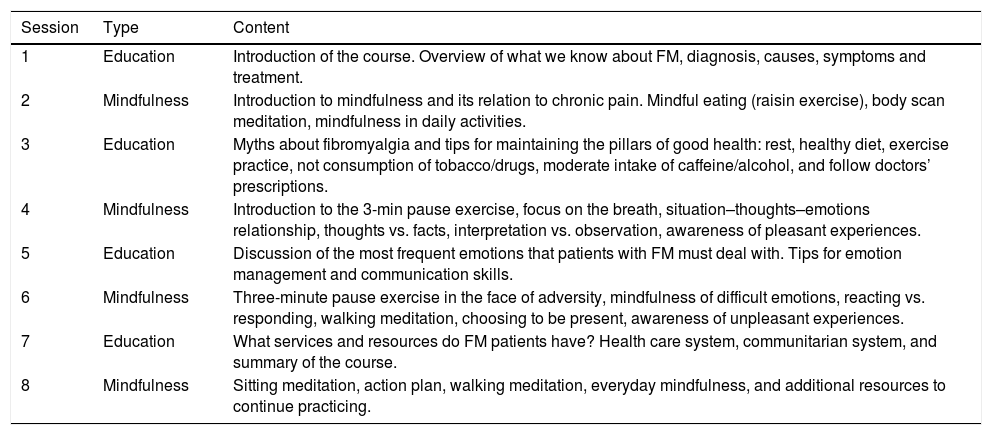
The MINDSET intervention consisted of four sessions psychoeducation about the FM, based on a previously validated program,14 and four sessions of mindfulness training, based on the Mindfulness-Based Stress Reduction curriculum.15 The sessions, which lasted about 2h and were conducted twice per week, were run by health psychologists in a group setting of 8–10 patients per group. The main targets of the intervention were: increase knowledge about FM, promotion of healthy habits, and fostering emotion regulation in face of adversity. This intervention was an add-on to the patient's usual care (usually, medication). No additional active treatments were provided. Table 1 presents a summary of the sessions.
Content of the sessions.
| Session | Type | Content |
|---|---|---|
| 1 | Education | Introduction of the course. Overview of what we know about FM, diagnosis, causes, symptoms and treatment. |
| 2 | Mindfulness | Introduction to mindfulness and its relation to chronic pain. Mindful eating (raisin exercise), body scan meditation, mindfulness in daily activities. |
| 3 | Education | Myths about fibromyalgia and tips for maintaining the pillars of good health: rest, healthy diet, exercise practice, not consumption of tobacco/drugs, moderate intake of caffeine/alcohol, and follow doctors’ prescriptions. |
| 4 | Mindfulness | Introduction to the 3-min pause exercise, focus on the breath, situation–thoughts–emotions relationship, thoughts vs. facts, interpretation vs. observation, awareness of pleasant experiences. |
| 5 | Education | Discussion of the most frequent emotions that patients with FM must deal with. Tips for emotion management and communication skills. |
| 6 | Mindfulness | Three-minute pause exercise in the face of adversity, mindfulness of difficult emotions, reacting vs. responding, walking meditation, choosing to be present, awareness of unpleasant experiences. |
| 7 | Education | What services and resources do FM patients have? Health care system, communitarian system, and summary of the course. |
| 8 | Mindfulness | Sitting meditation, action plan, walking meditation, everyday mindfulness, and additional resources to continue practicing. |
SPSS v22 was used for all statistical analyses. A positive/negative humor styles ratio was calculated to provide an index indicative of proportion of use of both types of humor styles. A linear regression (with step-wise method) was used to analyze the predictive effect of humor styles on the perceived clinical change after the intervention. A linear hierarchic regression was computed to assess the unique effect of humor styles after controlling by mindfulness scores. Spearman correlations were performed to evaluate associations between humor styles and clinical and mindfulness variables at baseline. Wilcoxon's test was then computed to analyze pre-post differences and Hedges’ g was used to calculate the effect size.
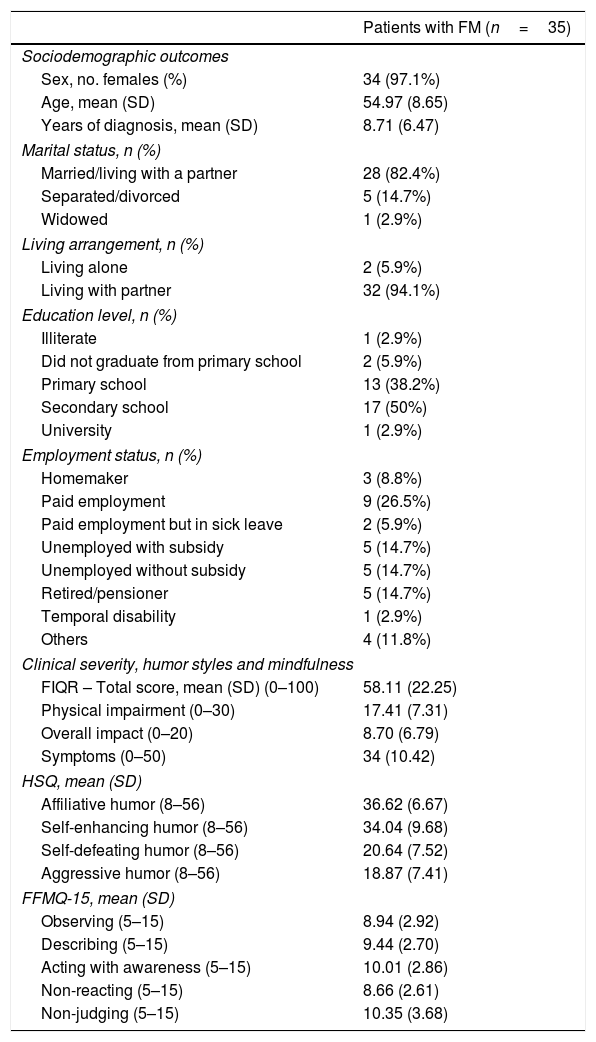
ResultsTable 2 presents the baseline data of the sample. Change in FIQR scores (i.e., functional impact of the FM) was not predicted by any humor style, but significant effects were found for the PGIC (i.e., perceived clinical change). In the case of perceived change in physical activity, affiliative humor emerged as a significant predictor (β=−0.395, F=4.44, R2=.156, P=.046); on the other hand, the positive/negative humor style ratio was a significant predictor of perceived change in work activity (β=−0.432, F=5.51, R2=.187, P=.027), mood (β=−0.454, F=6.22, R2=.206, P=.020), and pain (β=−0.498, F=7.90, R2=.248, P=.010). In addition, self-defeatinghumor significantly predicted the perceived change in pain (β=0.467, F=6.68, R2=.218, P=.016). All these effects were preserved after controlling for the mindfulness-facets.
Baseline characteristics of the participants.
| Patients with FM (n=35) | |
|---|---|
| Sociodemographic outcomes | |
| Sex, no. females (%) | 34 (97.1%) |
| Age, mean (SD) | 54.97 (8.65) |
| Years of diagnosis, mean (SD) | 8.71 (6.47) |
| Marital status, n (%) | |
| Married/living with a partner | 28 (82.4%) |
| Separated/divorced | 5 (14.7%) |
| Widowed | 1 (2.9%) |
| Living arrangement, n (%) | |
| Living alone | 2 (5.9%) |
| Living with partner | 32 (94.1%) |
| Education level, n (%) | |
| Illiterate | 1 (2.9%) |
| Did not graduate from primary school | 2 (5.9%) |
| Primary school | 13 (38.2%) |
| Secondary school | 17 (50%) |
| University | 1 (2.9%) |
| Employment status, n (%) | |
| Homemaker | 3 (8.8%) |
| Paid employment | 9 (26.5%) |
| Paid employment but in sick leave | 2 (5.9%) |
| Unemployed with subsidy | 5 (14.7%) |
| Unemployed without subsidy | 5 (14.7%) |
| Retired/pensioner | 5 (14.7%) |
| Temporal disability | 1 (2.9%) |
| Others | 4 (11.8%) |
| Clinical severity, humor styles and mindfulness | |
| FIQR – Total score, mean (SD) (0–100) | 58.11 (22.25) |
| Physical impairment (0–30) | 17.41 (7.31) |
| Overall impact (0–20) | 8.70 (6.79) |
| Symptoms (0–50) | 34 (10.42) |
| HSQ, mean (SD) | |
| Affiliative humor (8–56) | 36.62 (6.67) |
| Self-enhancing humor (8–56) | 34.04 (9.68) |
| Self-defeating humor (8–56) | 20.64 (7.52) |
| Aggressive humor (8–56) | 18.87 (7.41) |
| FFMQ-15, mean (SD) | |
| Observing (5–15) | 8.94 (2.92) |
| Describing (5–15) | 9.44 (2.70) |
| Acting with awareness (5–15) | 10.01 (2.86) |
| Non-reacting (5–15) | 8.66 (2.61) |
| Non-judging (5–15) | 10.35 (3.68) |
Note: FIQR: Fibromyalgia Impact Questionnaire – Revised; HSQ: Humor Styles Questionnaire; FFMQ-15: Five Facets Mindfulness Questionnaire – 15 item version; one patient did not attend to the first session; thus, the table presents data for 34 patients except for sex, age, and years of diagnosis.
Some significant correlations were found between humor styles, FIQR and mindfulness facets. The affiliative style presented significant negative correlations with FIQR scores (r=−.50, P=.004). No significant correlations were found with any of the mindfulness facets. The self-enhancing style presented a significant correlation with the FIQR symptoms subscale (r=−.38, P=.033), and with the mindfulness facets Describing (r=.50, P=.003), Acting with awareness (r=.37, P=.039), and Non-judging (r=.38, P=.033). The aggressive style correlated positively and significantly with the total FIQR score (r=.41, P=.021), and with the mindfulness facet Non-judging (r=−.44, P=.012). On the other hand, self-defeating humor did not correlate significantly with the FIQR nor with the FFMQ-15. Finally, when considering the humor styles ratio, significant correlations were found for the FIQR (r=−.54, P=.002) and, regarding mindfulness facets, with Acting with awareness (r=.36, P=.042) and with Non-judging (r=.58, P=.001).
Finally, and despite not being the main aim of this study, it needs to be noticed that the intervention achieved a notable degree of adherence (74% of attendance to the sessions) and was considered satisfactory (9/10), useful (8.9/10), recommendable (8.7) and non-aversive (0.5/10) by the participants in a post-treatment ad-hoc opinion survey. After the intervention, the mean FIQR score showed a significant 14% of improvement (P<.001), although the effect size was small (Hedges’ g=0.36). In the case of perceived changes after the treatment (PGIC; 1=much better, 4=no change, 7=much worse), overall small improvements were observed: mood (M=2.72, SD=1.31), social activity (M=2.93, SD=1.13), overall status (M=3.14, SD=0.83), physical activity (M=3.38, SD=0.86), work activity (M=3.41, SD=1.05), and pain (M=3.59, SD=0.91).
DiscussionTo date, this is the first study to assess the predictive role of humor styles in the perceived clinical changes of a mindfulness-based intervention for FM. Our analyses indicate some predictive effects for affiliative humor, self-defeating humor, and the ratio on different areas of the perceived clinical improvement. A possible explanation could be that those patients who scored higher in positive humor styles would probably present certain personality traits (e.g. openness to experience, psychological flexibility, self-efficacy, see Martin et al.3) which could facilitate to act on the suggestions and advice given during the sessions, such as practicing aerobic exercise; on the other hand, patients with higher levels of negative humor styles could also present higher levels of depressive symptomatology, lower self-efficacy and more external locus of control,16 which could hinder learning and implementing the practices addressed to reduce pain and its consequences. Therefore, an interesting challenge would be finding ways to increase the ratio of humor styles, particularly in those cases in which the ratio is lower than 1:1 (i.e., more frequent use of negative styles). Future studies could focus on testing interventions addressed to increasing this ratio and testing the clinical implications.
To our knowledge, the present pilot study is also the first to use the FFMQ to study the relationship between mindfulness and humor styles; our results indicate that self-enhancing humor is the most strongly mindfulness-related humor style, as it has been significantly associated with multiple facets. It is possible that these associations may be related to the ability to regulate emotions and accept negative emotional states that cannot be immediately changed.6 On the other hand, aggressive humor presented a significant negative correlation with Non-judging, which is defined as refraining from judgments or self-criticism about having certain experiences (e.g., feeling anxious).
Some limitations of the present study cannot be overlooked: the small number of patients and the absence of a control group hampered analyses and reduced the robustness of the results. The lack of other clinical, coping-related and mindfulness measures administered both at pre- and at post-intervention limited the soundness of the conclusions, which in most cases have an important hypothetical base. Future studies should also evaluate other aspects of humor such as humor production or appreciation, and these studies should be conducted considering the socio-cultural differences regarding humor that some studies have already assessed.17
In conclusion, the preliminary findings of this pilot study indicate that affiliative humor and the ratio of humor styles seem to be predictors of self-reported changes after the MINDEST intervention in different areas which are relevant for FM patients (e.g., pain, work, mood). These effects could be attributed to a better disposition in patients with positive humor styles to learn and implement the concepts and resources that the intervention offered. Also, the self-enhancing humor appeared to be related to a number of mindfulness facets. Despite the considerable limitations of this study, these preliminary results contribute to knowledge on the link between humor and chronic pain and suggest some lines of research which could be undertaken in future studies.
FundingThe study has been funded in part by the Instituto de Salud Carlos III (ISCIII), Ministry of Economy and Competitiveness (Spain) through the Network for Prevention and Health Promotion in Primary Care (RD16/0007/0012), by a grant for research projects in health from ISCIII (PI15/00383) co-financed with European Union ERDF funds. The first listed author has a FI predoctoral contract awarded by the Agency for Management of University and Research Grants (AGAUR; 2017; FI_B00754). The third listed author has a “Sara Borrell” research contract from the ISCIII (CD16/00147). The fourth listed author has a FI predoctoral contract awarded by the Agency for Management of University and Research Grants (AGAUR; 2018; FI_B00783). The last listed author (JVL) has a “Miguel Servet” research contract from the ISCIII (CP14/00087).
Conflict of interestThe authors declare no conflicts of interest.


