


To analyze the effects of mud therapy on perceived pain, Health Related Quality of Life (HRQL) and drug use in patients diagnosed with knee osteoarthritis.
Material and methodsA prospective, controlled clinical trial. The sample (n=147) was divided into an experimental group (EG) of 61 subjects (69.13±5.60 years) who received 11 consecutive sessions of peloids in the knee/s affected by the process described and a control group (CG) of 60 subjects (73.08±8.90 years) who continued routine drug treatment. The sample was assessed before and after intervention using the SF-36, visual analog scale and changes in drug use, setting a significance level of P≤.05.
ResultsAfter the intervention, there were statistically significant differences (P<.05) in all parameters analyzed between EG and CG, reduced drug use in the EG versus no change in the CG. The general health, bodily pain and perceived pain are those that show major changes between the two groups.
ConclusionsMud therapy in patients diagnosed with knee osteoarthritis attains immediate effects on perceived pain and HRQOL, reducing the consumption of specific drugs. Studies are needed to evaluate the scientific evidence from the effects of such intervention.
Analizar los efectos de la terapia con peloides sobre el dolor percibido, la calidad de vida relacionada con la salud (CVRS) y el consumo de medicamentos en sujetos diagnosticados de osteoartritis de rodilla.
Material y métodosEnsayo clínico prospectivo y controlado. La muestra (n=147) fue dividida en un grupo experimental (GE) de 61 sujetos (69,13±5,60 años), que recibió 11 sesiones consecutivas de peloides en la rodilla afectada según el procedimiento terapéutico descrito, y un grupo control (GC) de 60 sujetos (73,08±8,90 años), que continuó con su tratamiento farmacológico rutinario. La muestra fue valorada antes y después de la intervención mediante el cuestionario SF-36, la escala visual analógica y la evolución en el consumo de medicamentos, estableciendo el nivel de significación para p≤0,05.
ResultadosTras finalizar la intervención, existieron diferencias estadísticamente significativas (p<0,05) en todas las variables analizadas entre el GE y GC, reduciéndose el consumo de medicamentos en el GE frente a la ausencia de cambios en el GC. Las dimensiones salud general, dolor corporal y el dolor percibido son las que muestran mayores cambios entre ambos grupos.
ConclusionesLa peloterapia en pacientes diagnosticados de osteoartritis de rodilla obtiene efectos inmediatos sobre el dolor percibido y la CVRS, reduciendo el consumo de medicamentos específicos. Son necesarios estudios evalúen desde la evidencia científica los efectos de dicha intervención.
The term Peloid refers to all those natural products consisting of a mixture of a mineral-water or mineromedicinal (including sea or salt lake water) with inorganic or organic materials resulting from geological, biological or both processes used simultaneously with a therapeutic purpose and applied as wrapping or bath.1 The external application of all or part of these products is called pelotherapy, it being a therapeutic modality that, despite having defined mechanisms of action, route and site of different application, is still under the umbrella of balneotherapy, hydrotherapy and spa treatment.2
The application of peloids in rheumatic diseases has been widely used since ancient times, constituting an unquestionable reality, even when and despite having proven their therapeutic efficacy in various rheumatic processes,3–7 there are few studies evaluating the clinical effects resulting from its application in knee osteoarthritis (OAR).8
Several studies have analyzed and compared the effectiveness of pelotherapy in patients diagnosed with OA of the knee (OAK)9–11 versus other intervention procedures5,12 in the short and medium term, such as drug or rehabilitation13–15 or,16–18 noticing improvements in perceived pain, functional capacity, quality of life or drug use; however, the effects of peloid treatment are often masked by it not being applied in isolation.7
At present, despite the fact that the main mechanism of action is known to be thermotherapeutic, other studies have shown systemic activity through changes observed in biochemical and molecular parameters, such as reduced plasma α tumor necrosis factor, IL-1β, IL-1, IL-6, PGE2, LTB419–21 responsible for the reduction of pain and inflammatory processes, increases in the synthesis of noradrenaline, cortisol, beta-endorphins and insulin growth factor, due to the thermal stress caused and stimulating the metabolism of chondrocytes producing joint cartilage protective effects9,11 and inhibition in free radical synthesis by influencing antioxidant reactions.21
Given the need to know from a scientific standpoint, the effects reported by peloid therapy, the main objective of this study was to determine the effects of pelotherapy in perceived pain, quality of life related to health (HRQOL) and trends in drug use in patients diagnosed with OAK versus a control group that continues its routine drug treatment.
Materials and MethodsPatient SelectionA total of 147 patients with OAK participated voluntarily in this open, randomized and controlled clinical trial. Inclusion criteria were established as follows: age between 65 and 80 years and being diagnosed with OAK according to the American College of Rheumatology,22 criteria; we excluded patients with partial or total knee prosthesis, those who received physiotherapy in the past 2 weeks or intra-articular injections in the past 6 months and those whose cognitive state made data collection difficult, leaving a final sample of 132 subjects (96 women and 36 men), of whom 11 were lost to follow up (Fig. 1).

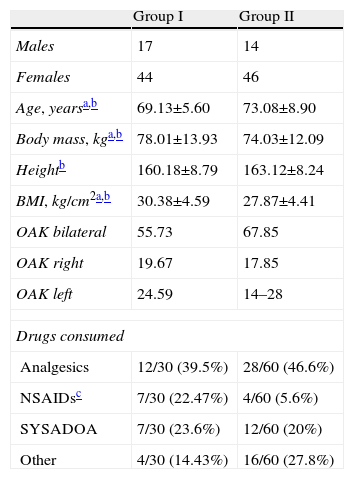
The sample consisted of patients referred by their National Health System primary care physician (PCP) diagnosed with OAK to the Balneario El Raposo (Badajoz, Spain) through the Social Hydrotherapy Program offered by the Government of Spain IMSERSO (experimental group n=61) and those who, despite being diagnosed with OAK by their central PCP in Mejostilla (Cáceres, Spain), were not referred (control group n=60). The demographic characteristics of the sample are presented in Table 1.
Sociodemographic Characteristics of the Sample at Baseline.
| Group I | Group II | |
| Males | 17 | 14 |
| Females | 44 | 46 |
| Age, yearsa,b | 69.13±5.60 | 73.08±8.90 |
| Body mass, kga,b | 78.01±13.93 | 74.03±12.09 |
| Heightb | 160.18±8.79 | 163.12±8.24 |
| BMI, kg/cm2a,b | 30.38±4.59 | 27.87±4.41 |
| OAK bilateral | 55.73 | 67.85 |
| OAK right | 19.67 | 17.85 |
| OAK left | 24.59 | 14–28 |
| Drugs consumed | ||
| Analgesics | 12/30 (39.5%) | 28/60 (46.6%) |
| NSAIDsc | 7/30 (22.47%) | 4/60 (5.6%) |
| SYSADOA | 7/30 (23.6%) | 12/60 (20%) |
| Other | 4/30 (14.43%) | 16/60 (27.8%) |
NSAIDs: nonsteroidal antiinflammatory drugs, BMI: body mass index; OAK: knee osteoarthritis; SYSADOA: chondroprotective drugs.
The study was approved by the Bioethics Committee of the University of Extremadura and informed consent was obtained from participants.
Randomization of the sample in each group was performed by using the randomization function «RANDBETWEEN (1, 2)» of the Microsoft Excel 2007 program, including those in the study who were randomly assigned by the number 1. II or control group who received no intervention, continuing their routine drug therapy for the duration of the study, as well as the experimental group. The experimental group received 11 I or daily sessions of peloids, according to the therapeutic procedure implemented by their health care professionals. This consists of an application of peloid by brush 30°C, followed by a drying period of 30min in the solarium spa. Subsequently, patients received a thermal water bath for 15min with peloid, ending with the removal of the same with a thermal jet for 2min. The total duration of the intervention was 47min, conducted by the same therapists the Spa, with over 10 years experience in the application of this technique. Both the professionals who performed the technique as the evaluator of the variables analyzed were unaware of the purpose of the study, the latter being independent to the Spa center.
The peloid of Balneario El Raposo (Badajoz, Spain) is obtained directly from a natural stream, with optimal chemical and thermophysical properties for application after a month of ripening and at a temperature between 20 and 30°C. It contains mainly calcite, silica, sodium feldspar (albite) and potassium feldspar (orthoclase), the most common being inorganic SiO2, LOI, Al2O3 and CaO. Its mineral waters contain high levels of chlorine, sodium, calcium and bicarbonate. They are of medium mineralization and emerge at 16.3°C. Their anions contain chlorine (87.3mg/l), bicarbonates (386.3mg/l) and sodium cations (51.7mg/l) and calcium (133.2mg/l).
RatingsThe evaluator assessed each of the subjects’ perceived pain intensity using a visual analog scale (VAS). This method assigns a score from 0 (complete absence of pain) to 10 (maximum pain). HRQL was measured also by the SF-36.23 It consists of 36 questions, divided into eight dimensions of quality of life (physical function, physical role, pain, vitality, social function, emotional role, mental health and general health), so that the higher the score, the better the quality of life. Finally, we quantified the type of drug consumed and its evolution in intake during the intervention through organized records. The assessment for each of the subjects was done just before the intervention (baseline assessment) and after the last session (final assessment), and with a period of 11 days between the two.
Statistical AnalysisThe study sample was calculated by the sample size program “G-Power 3.1.2”, with the following parameters: a statistical significance of P<.05, study power of 80% (0.8) for two study groups and a medium effect size of f=0.25.
Subsequently, a descriptive analysis of each of the variables, showing their mean values and standard deviations was performed. To determine if the sample followed a normal distribution and statistical equivalence existed between groups in demographic variables we performed the Shapiro–Wilks test and compared by one-way ANOVA. After determining that the sample followed a normal distribution, we compared the values obtained at baseline and at the end for each test variable using the Student's t-test for paired samples. To compare the effects obtained after surgery between groups (experimental group vs Controls) we analyzed the sample using an independent sample test or Student's t test, Mann–Whitney U (depending on whether the variances were considered homogeneous populations or no).
To analyze the variable ‘drug use’ we used contingency tables, using the Pearson's chi-square test after verifying the conditions of validity.
In addition, we calculated the effect size (effect size) of each intervention by Cohen's d coefficient. A value greater than 0.8 was considered high, 0.5 moderate and less than 0.2 was considered low.24 The level of significance was set at a P value <.05. Data analysis was performed using SPSS software, version 19.0.
ResultsMean values±standard deviation of demographic variables analyzed are shown in Table 1, showing equivalence (P≥.05) in the two groups for all of them, except for the subjects consuming nonsteroidal antiinflammatory drugs (NSAIDs), where statistically significant differences were observed.
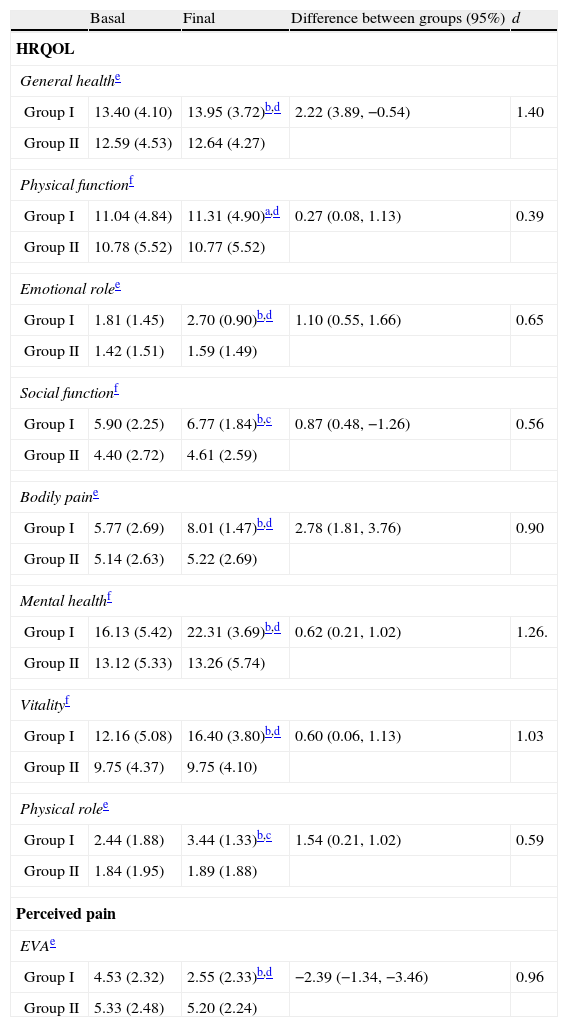
The patients in the experimental group had statistically significant improvements from baseline to the final assessment (P<.05), both in the variable of perceived pain as in all HRQoL dimensions analyzed, with a medium-large effect size for all them (Table 2). In the control group, there were no statistically significant improvements (P≥.05) in any of the variables under study.
Results of Statistical Comparison Between Groups of the Analyzed Dimensions of HRQOL and Perceived Pain After 11 Days of Intervention.
| Basal | Final | Difference between groups (95%) | d | |
| HRQOL | ||||
| General healthe | ||||
| Group I | 13.40 (4.10) | 13.95 (3.72)b,d | 2.22 (3.89, −0.54) | 1.40 |
| Group II | 12.59 (4.53) | 12.64 (4.27) | ||
| Physical functionf | ||||
| Group I | 11.04 (4.84) | 11.31 (4.90)a,d | 0.27 (0.08, 1.13) | 0.39 |
| Group II | 10.78 (5.52) | 10.77 (5.52) | ||
| Emotional rolee | ||||
| Group I | 1.81 (1.45) | 2.70 (0.90)b,d | 1.10 (0.55, 1.66) | 0.65 |
| Group II | 1.42 (1.51) | 1.59 (1.49) | ||
| Social functionf | ||||
| Group I | 5.90 (2.25) | 6.77 (1.84)b,c | 0.87 (0.48, −1.26) | 0.56 |
| Group II | 4.40 (2.72) | 4.61 (2.59) | ||
| Bodily paine | ||||
| Group I | 5.77 (2.69) | 8.01 (1.47)b,d | 2.78 (1.81, 3.76) | 0.90 |
| Group II | 5.14 (2.63) | 5.22 (2.69) | ||
| Mental healthf | ||||
| Group I | 16.13 (5.42) | 22.31 (3.69)b,d | 0.62 (0.21, 1.02) | 1.26. |
| Group II | 13.12 (5.33) | 13.26 (5.74) | ||
| Vitalityf | ||||
| Group I | 12.16 (5.08) | 16.40 (3.80)b,d | 0.60 (0.06, 1.13) | 1.03 |
| Group II | 9.75 (4.37) | 9.75 (4.10) | ||
| Physical rolee | ||||
| Group I | 2.44 (1.88) | 3.44 (1.33)b,c | 1.54 (0.21, 1.02) | 0.59 |
| Group II | 1.84 (1.95) | 1.89 (1.88) | ||
| Perceived pain | ||||
| EVAe | ||||
| Group I | 4.53 (2.32) | 2.55 (2.33)b,d | −2.39 (−1.34, −3.46) | 0.96 |
| Group II | 5.33 (2.48) | 5.20 (2.24) | ||
d: Cohen's d coefficient.
Values are presented as mean±standard deviation at the beginning and at the end (after 11 consecutive days) and the average difference between groups (95% confidence interval).
In the final assessment, both parametric Student's t test and the nonparametric Mann–Whitney test showed statistically significant differences between groups (P<.05), highlighting the dimensions seen in “general health” and “body pain” and “perceived pain” as measured by the VAS (Table 2).
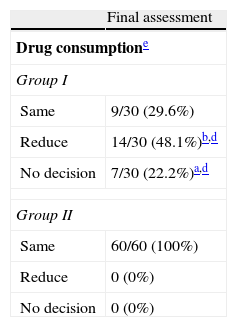
Regarding changes in drug consumption, a reduction and a significant absence in the intake was observed for the experimental group (Table 3), who used the most analgesics in both groups, followed by chondroprotective drugs in the experimental group and ‘others’, such as opioid analgesics or topical drugs in the control group (Table 3).
Results Regarding Changes in Drug Use Between Group I vs Group II After 11 Days of Intervention.
| Final assessment | |
| Drug consumptione | |
| Group I | |
| Same | 9/30 (29.6%) |
| Reduce | 14/30 (48.1%)b,d |
| No decision | 7/30 (22.2%)a,d |
| Group II | |
| Same | 60/60 (100%) |
| Reduce | 0 (0%) |
| No decision | 0 (0%) |
Values are presented as percentages.
The main objective of this study was to determine the effects derived after application of natural peloid on perceived pain, HRQoL and consumption of drugs in people diagnosed with OAK.
The results showed statistically significant improvements in all parameters analyzed for the experimental group, with a medium-large effect size in all items analyzed.
Until recently, pelotherapy is a procedure used in rheumatic diseases derived from empiricism and intuitive reasoning. This has resulted in its lack of inclusion as an effective intervention in models of care and evidence-based clinical guidelines for the management of OAK.25
At present, studies such as Pnevmatikatos et al.,4 Cantarini et al.,5 or Fraioli et al. have analyzed10 the therapeutic effect reported by different peloids therapy by patients with OAK in spas. Other comparisons have been conducted on the effectiveness of pelotherapy against other measures based on thermotherapy, such as hot-packs,17 and magnetic fields, such as shortwave5,16 or other therapeutic modalities applied in spas,18 with minor works comparing their influence over drug therapy,13,16 like Odabasi et al.,26 a study very similar from the methodological point of view to ours.
Regarding the variables analyzed after applying pelotherapy in OAK highlights perceived pain as the most studied symptom. Rates of improvement achieved match the results reported in previous studies3,10,13,17,26 after being applied in isolation. Other authors also obtained results combining peloid with a thermal bath or exercise.15,18,19
Regarding HRQoL, we agree with several authors in observing the positive influence of this intervention on quality of life.7,15,17 The results are in line with those reported by Forestier et al.,15 after applying Peloids and thermal bath for 3 weeks in a sample 118 subjects, using the same measurement instrument that we used in the present work. Until now the effect of treatment with physical exercise on pain and functional capacity in OAK was well known27,28; however, and after the results are shown, there could be improvements in the dimensions related to the psychobiological field, such as mental health vitality and the emotional role as emerging psychosocial factors in group therapy within the right context in which it is applied and having a decisive influence on the improvement in dimensions related to mental health.29
It is for this reason that future research should explore its potential efficacy in the treatment of depressive symptoms in older people with changes in HRQoL30 and its direct influence on the habitual use of specific drugs; there are currently a very small number of studies analyzing the influence of pelotherapy on these variables.
Likewise, we agree with Fioravanti et al.,11 on the need for longer follow-up periods in order to know the scope of the technique and ensure better medium to long term results as,5,10 being one of the limitations of this study.
In short, peloids therapy in patients diagnosed with OAK obtains immediate effects on perceived pain and HRQOL, reducing the consumption of specific drugs. Studies are needed to evaluate the scientific evidence from the effects of the intervention, establishing uniform criteria applying them as regards the duration, frequency and optimum temperature of peloid.
Ethical ResponsibilitiesProtection of People and AnimalsThe authors declare that procedures conformed to the ethical standards of the committee responsible for human experimentation and were in accordance with the World Medical Association Declaration of Helsinki.
Confidentiality of DataThe authors declare that they have followed the protocols of their workplace on the publication of data from patients and all patients included in the study have received sufficient information and gave their written informed consent to participate in this study.
Right to Privacy and Informed ConsentThe authors state that no patient data appears in this article.
DisclosuresThe authors have no disclosures to make. The undersigning authors state their authorship of this study, accepting the journals publication norms and transfer their rights to Reumatología Clínica, them being original and inedit.
Please, cite this article as: Espejo Antúnez L, et al. Efectos de la terapia con peloides sobre el dolor percibido y la calidad de vida relacionada con la salud en pacientes con osteoartritis de rodilla. Reumatol Clin. 2013. http://dx.doi.org/10.1016/j.reuma.2012.09.005.


