





A 50-year-old male came to the emergency room with fever and pain in the left foot for the past 10h. He had no history of trauma.
On physical examination we found erythema, and warm, tender swelling of the distal forefoot with pain intensified by flexion of the third toe.
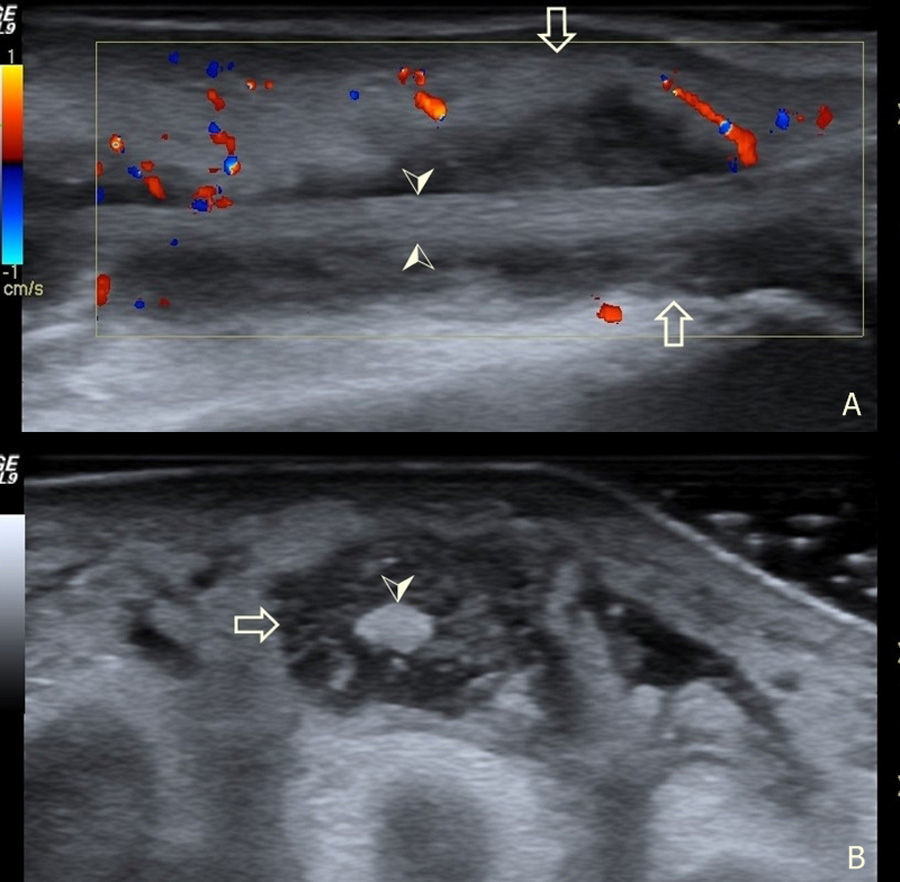
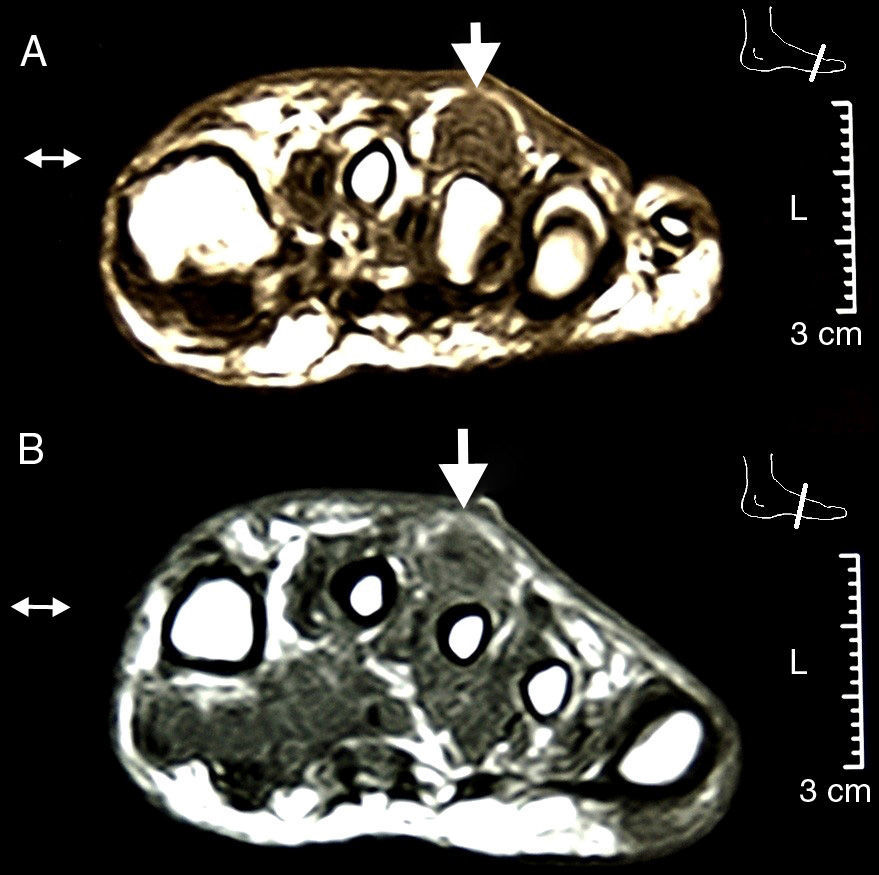
An ultrasound of the foot determined the presence of an hypoechoic effusion into the sheath of the extensor of the third toe at the middle and distal thirds with moderate color Doppler signal and no increase in skin thickness (Fig. 1). Since usually branches of the digitorum extensor have no sheath beyond the middle third of the forefoot1 we confirmed the diagnosis with an MRI (Fig. 2). We started antibiotic treatment with vancomycin from the first contact, and debridement was performed on the second day, draining 12cc of purulent-looking fluid from which we identified a strain of Staphylococcus aureus, which coincided with the results of blood cultures.
Infectious tenosynovitis of the foot occurs most often at the plantar flexors and is related to cutaneous perforation by foreign bodies,2 a very rare presentation is on the foot extensor region. Mechanical tenosynovitis of the extensor tendons is usually associated with chronic exposure to repeated trauma3 that occurs in the ultramarathoner foot syndrome due to mechanical contact between the tendon and proximal osteophitic prominence wedges.4 Cellulitis of the dorsum of the foot is the first differential diagnosis. The diagnosis can be made through ultrasound5 visualizing the tendon sheath immersed in a hypoechoic fluid and confirmed through aspiration and microbiological study. MRI can also assess the existence of6,7 bone involvement. Antibiotic treatment should be started before the diagnostic suspicion, although the duration and route of administration is heterogeneous in the few similar case reports found.8–10 In our opinion, systemic compromise justifies intravenous antibiotic treatment.
Ethical ResponsibilitiesProtection of people and animals. The authors state that no experiments were performed on humans or animals.Data confidentiality. The authors declare that they have followed the protocols of their workplace regarding the publication of data from patients and all patients included in the study have received sufficient information and gave their written informed consent to participate in this study.Right to privacy and informed consent. The authors have obtained informed consent from patients and/or subjects referred to in the article. This document is in the possession of the author of correspondence.
DisclosuresThe authors have no disclosures to make.
Please, cite this article as: Guillén Astete C, et al. Tenosinovitis infecciosa del aparato extensor del pie. Reumatol Clin. 2014;10:56–57.


