




In Spain, the prevalence of different rheumatic diseases is known mainly through the EPISER studies coordinated by the Spanish Society of Rheumatology and based on surveys in a population sample. The aim of our study is to describe the prevalence in 2016 of different rheumatic diseases in the population residing in Baix Empordà according to healthcare coding records.
Materials and methodsObservational, descriptive and cross-sectional study carried out on the population attended from 2016 to 2017 in SIBBE (Serveis de Salut Integrats del Baix Empordà), an organizational service that includes all the healthcare facilities in the Baix Empordà area with a unique information system. Patients ≥ 20 years of age were selected and the ICD9-CM coding of all their healthcare contacts was analysed according to 11 entities and 28 diseases. The entities were: polyarthritis, spondyloarthritis, microcrystalline arthritis, osteoarthritis, soft tissue rheumatism, fibromyalgia, chronic spinal pain, osteoporosis, connective tissue diseases, vasculitis and others. The studied population was assigned to the categories: "with rheumatic disease", "possible rheumatic disease" and "without rheumatic disease".
ResultsIn total, 71,785 patients were distributed as: 36.2% “with rheumatic disease (n = 25,990); 6.1% with “possible rheumatic disease” (n = 4406) and 57.7% “without rheumatic disease” (n = 41,389). The group "with rheumatic disease" showed a predominance of women (59.7% vs. 44.9%) and older age (59.1 ± 17.7 vs. 45.1 ± 16.2; p < .001) compared to the group "without rheumatic disease". The presence of rheumatic disease increased progressively with age, being maximum in the group between 55–75 years.
Conclusions36.2% of our population has some type of rheumatic disease. The estimated prevalence of some rheumatic diseases in the Baix Empordà population is partially consistent with that estimated by the EPISER 2016 study. Rheumatic disease affects women in a greater proportion and is more frequent in patients over 45 years of age.
En España, la prevalencia de diferentes enfermedades reumáticas se conoce principalmente a través de los estudios EPISER coordinados desde la Sociedad Española de Reumatología y que parten de encuestas en una muestra poblacional. Nuestro estudio tiene por objetivo describir la prevalencia en 2016 de las distintas enfermedades reumáticas en la población residente en el Baix Empordà según registros de codificación asistencial.
Materiales y métodosEstudio, observacional, descriptivo y transversal realizado sobre la población residente durante los años 2016–2017 en la comarca del Baix Empordà, donde una organización sanitaria integrada (Serveis de Salut Integrats Baix Empordà, SSIBE) gestiona todos los dispositivos asistenciales públicos con un sistema de información unificado. Se seleccionaron los pacientes ≥ 20 años y se analizó la codificación CIE-9-CM de sus contactos asistenciales en función de 11 agrupaciones diagnósticas de 28 enfermedades reumáticas. Las agrupaciones fueron: poliartritis, espondiloartritis, artritis microcristalinas, artrosis (excepto localización vertebral), reumatismos de partes blandas, fibromialgia, dolor vertebral crónico (incluyendo artrosis), osteoporosis, enfermedades del tejido conectivo, vasculitis y otros. La población estudiada se asignó a tres categorías: «con enfermedad reumática», «posible enfermedad reumática» y «sin enfermedad reumática».
ResultadosLa muestra final fue de 71.785 personas, así distribuidas: «con enfermedad reumática»(n = 25.990; 36,2%); «posible enfermedad reumática» (n = 4.406; 6,1%) y «sin enfermedad reumática» (n = 41.389; 57,7%). El grupo «con enfermedad reumática» mostró un predominio de mujeres (59,8% vs. 44,9%) y mayor edad (59,1 ± 17,7 vs. 45,1 ± 16,2; p < 0,001) en comparación al grupo «sin enferme-dad reumática». La presencia de enfermedad reumática aumentó progresivamente con la edad, siendo máxima en el grupo de 55–75 años.
ConclusionesEl 36,2% de nuestra población presenta algún tipo de enfermedad reumática. La prevalencia estimada de varias enfermedades reumáticas en la población del Baix Empordà coincide parcialmente con la estimada por el estudio EPISER 2016. La enfermedad reumática afecta en mayor proporción a mujeres, y es más frecuente en pacientes con edad superior a 45 años.
Rheumatic diseases are the second most frequent cause of consultation in the European Union, with one in five inhabitants receiving chronic treatment for a disease of this type.1 According to Eurobarometer 2007,2 22% of the European population has suffered from a chronic musculoskeletal disease, and these conditions are responsible for 32% of the chronic treatments prescribed. Pain is a frequent symptom and one of the main reasons for associated disability, being chronic and limiting in 25% of affected people.2
In Spain, the prevalence of different rheumatic diseases is mainly known through the EPISER studies, coordinated by the Spanish Society of Rheumatology. The latest of these, EPISER 20163,4 provides data on the prevalence of several rheumatic diseases in Spain, including rheumatoid arthritis, ankylosing spondylitis, systemic lupus erythematosus and symptomatic osteoarthritis in several locations. This study revealed a prevalence of 28.9% of medical consultations for osteoarticular problems in a representative sample of the general adult population in Spain.4,5
The "Analysis and improvement of hospital and healthcare processes" project began in 2012 as an initiative in which a group of managers, healthcare professionals and patients, using a specific methodology, made proposals for the improvement of healthcare processes with the aim of contributing to the efficiency of the system and improving the quality of care.6 Its 6th edition, which began in 2016, included the project "Analysis and improvement of hospital and healthcare processes, rheumatology". This is where a project is framed, promoted by the Catalan Society of Rheumatology to assess the complexity of care for rheumatic diseases. It was developed on the population of Baix Empordà, given that this area has proven experience in the analysis of the morbidity based on an integrated information system that includes the entire continuum of care.7 The first part of this project is the objective of this study: to describe the prevalence of the different rheumatic diseases in the population residing in Baix Empordà, a district in north-eastern Spain, during 2016 according to healthcare coding records.
Material and methodshe Baix Empordà is a district located in the northeast of Spain, in the province of Girona, in a coastal area (Costa Brava), which in 2016 had8: a life expectancy at birth of 80.2 years for men and 85.8 for women (80.4 and 86.2 respectively in Spain),9 a gross domestic product per inhabitant of 21,500 euros (23,980 euros in Spain10 and 73% of the population employed in the services sector (76.2% in Spain).11
Serveis de Salut Integrats del Baix Empordà (SSIBE) is an integrated healthcare organisation that manages all public healthcare services in the district, with the exception of primary care in one of the five basic health areas and mental health services. SSIBE covers the healthcare of 92,000 people and has an integrated information system for all its centres, which feeds a database containing the healthcare, economic and administrative information of all the people attended.12,13
This observational, descriptive and cross-sectional study was conducted on the resident population during 2016–2017 (people present in at least one of the two years) in the four basic health areas (ABS) managed by SSIBE (ABS la Bisbal d'Empordà, ABS Torroella de Montgrí, ABS Palafrugell and ABS Palamós) as well as in the Hospital de Palamós, a basic general hospital. The data used included single or multiple coding of cases in primary care, specialised outpatient care (outpatient and day hospital), acute hospitalisation, socio-health care, emergency and urgent care. Patients aged 20 years or older were selected and the ICD-9-CM coding of all their healthcare contacts with SSIBE was analysed.
A total of 302 ICD-9-CM codes corresponding to 28 different diseases were selected as possible and grouped into 11 different disease entities. The entities were: polyarthritis, spondyloarthritis, microcrystalline arthritis, osteoarthritis (except vertebral location), soft tissue rheumatism, fibromyalgia, chronic vertebral pain (including osteoarthritis), osteoporosis, connective tissue diseases, vasculitis and others. This selection is based on lists previously used in other publications, as well as on the SSIBE coding criteria set for its professionals.14,15 The ICD-9-CM codes as well as the groupings made are included in the Supplementary material (Appendix A).
The selection process was conducted in two phases. The first included the entire population that had been assigned any of the selected ICD-9-CM codes in the years 2013−2017. The SSIBE coding database, the register of confirmed visits to the rheumatology outpatient clinic and the register of dispensing of hospital-administered medicines were used. In this way, a prior classification by disease and pathological entity was made for everyone. After this initial selection, the following criteria were applied for the definitive identification and counting of patients in each of the categories used: verification of attendance in the study period (2016−17), elimination of duplicates (existence of several codes for the same entity), verification of being treated for one or more pathological entities during the study period, elimination of coding errors or unconfirmed diagnostic suspicion (presence of an isolated code without clinical follow-up after 2016 or not confirmed in the referral to specialised care). Patients from other areas or not included in the study population, patients who died before 2016 and those with a diagnosis of rheumatic disease onset after 2016 were excluded.
The entire study population was finally assigned to one of the following categories: "with rheumatic disease", "possible rheumatic disease" and "without rheumatic disease". Within the category of "possible rheumatic disease", those patients were included in whom isolated ICD-9-CM codes were identified, but in whom continued attendance for that health problem was not confirmed or was ruled out after study. This category was not used for the final analysis.
Microsoft Access™, Microsoft Excel™ and IBM SPSS™ version 25 was used for data management. Univariate analysis was performed, presenting qualitative variables by frequency and percentage, and quantitative variables with measures of central tendency; as well as bivariate analysis with chi-square and Student's t-square, with significance p < .05.
The study project was approved by the SSIBE Clinical Research Committee. The committee waived the requirement to obtain informed consent as the study was based on retrospective review of clinical-administrative records, without intervention of any kind. The data were extracted by a SSIBE professional from outside the research team and were managed in an anonymised form.
ResultsThe resident population in the territory managed by SSIBE was 91,130 people in 2016 and 92,050 in 2017. Of these, once the purification criteria had been applied, the population aged over 20 years was 71,785 people present in at least one of the two years, 36,381 women and 35,404 men.
The distribution in the established categories was: persons "with rheumatic disease" (n = 25,990; 36.2%); with "possible rheumatic disease" (n = 4406; 6.1%) and "without rheumatic disease" (n = 41,389; 57.7%).
The group "with rheumatic disease" included 15,541 women (59.8%), with a mean age of 60.1 years (SD 17.9) and 10,449 men of 57.6 years (SD 17.3) (statistically significant difference, p < .001). The group "without rheumatic disease" included 18,587 women (44.9%) and 22,802 men, with a mean age of 44.3 years (SD 16.4 years) and 45.8 years (SD 16.1) respectively, also a significant difference (p < .001). The group "with rheumatic disease" showed higher age than the group without disease (59.1 ± 17.7 vs. 45.1 ± 16.2; p < .001). The presence of females in the group "with rheumatic disease" (59.8%) and in the group "without rheumatic disease" (44.9%) represents a difference of 14.9%. The proportion of women was significantly different (p < .001) with the risk of having rheumatic disease in women being 1.33 (95% CI 1.31–1.35).
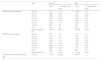
The presence of rheumatic disease increased progressively with age. Patients with rheumatic disease had a median and interquartile range of 59 years (46–73) vs. 43 years (33–55) in patients without rheumatic disease. Table 1 shows the age and sex distribution of the groups with and without rheumatic disease.
Distribution by age and sex of the groups analysed: “with rheumatic disease” and “without rheumatic disease”.
| Age | Women | Men | |||
|---|---|---|---|---|---|
| Total | % of people ≥20 years | Total | % of people ≥20 years | ||
| Without rheumatic disease | 20−24 y | 1733 | 2.4% | 1906 | 2.7% |
| 25−34 y | 4026 | 5.6% | 4214 | 5.9% | |
| 35−44 y | 4859 | 6.8% | 5741 | 8.0% | |
| 45−54y | 3533 | 4.9% | 4681 | 6.5% | |
| 55−64 y | 2116 | 2.9% | 3020 | 4.2% | |
| 65−74 y | 1238 | 1.7% | 1925 | 2.7% | |
| 75−84 y | 638 | .9% | 933 | 1.3% | |
| >84 y | 444 | .6% | 382 | .5% | |
| Subtotal without RD | 18,587 | 25.9% | 22,802 | 31.8% | |
| With rheumatic disease | 20−24 y | 303 | .4% | 271 | .4% |
| 25−34 y | 1075 | 1.5% | 755 | 1.1% | |
| 35−44 y | 1966 | 2.7% | 1599 | 2.2% | |
| 45−54y | 2,691. | 3.7% | 1973 | 2.7% | |
| 55−64 y | 2891 | 4.0% | 2023 | 2.8% | |
| 65−74 y | 2818 | 3.9% | 1807 | 2.5% | |
| 75−84 y | 2329 | 3.2% | 1412 | 2.0% | |
| >84 y | 1468 | 2.0% | 609 | .8% | |
| Subtotal with RD | 1541 | 21.6% | 10,449 | 14.6% | |
| Subtotal of those over 20 years of age | 34.128 | 47.5% | 33,251 | 46.3% | |
The prevalence of the different diseases is shown in Table 2, with the most prevalent entities being chronic vertebral pain (19%), soft tissue rheumatism (10.03%), osteoarthritis (9.62%) and osteoporosis (4.06%). Within chronic vertebral pain, lumbar pain was observed in 15.52% of the population studied, and cervical pain in 7.14% (without a diagnosis of osteoarthritis in these cases). Lumbar osteoarthritis and knee osteoarthritis – the most prevalent locations – obtained values of 3.96% and 3.6%, respectively.
Total prevalence and by subtypes of rheumatic diseases in patients resident at Serveis de Salut Integrats del Baix Empordà (SSIBE), 2016.
| SSIBE population | 2016 EPISER population | |||
|---|---|---|---|---|
| 71.785 people | 4.916 people | |||
| Prevalence of rheumatic diseases | 36,2% (25,990 cases) | 28.9% (1465 cases)% | ||
| N | % | Cases/100,000 inhabitants | % (95%confidence interval) | |
| Polyarthritis | 681 | .95% | 949 | |
| Rheumatoid arthritis | 488 | .68% | 680 | .82% (.59−1.15) |
| Other oligopolyarthritis | 193 | .27% | 269 | |
| Spondyloarthritis | 557 | .78% | 776 | |
| Ankylosing spondylitis | 284 | .40% | 396 | .26% (.14−.49) |
| Psoriatic arthritis | 223 | .31% | 311 | .58% (.38−.87) |
| Relative arthritis | 1 | .00% | 1 | |
| Undifferentiated spondiloarthritis | 49 | .07% | 68 | |
| Microcrystalline arthritis | 1398 | 1.95% | 1947 | |
| Gout | 1243 | 1.73% | 1732 | 2.40% (1.95−2.95) |
| Others | 155 | .22% | 216 | |
| Osteoarthritis | 6903 | 9.62% | 9616 | |
| Osteoarthritis of the hands | 885 | 1.23% | 1233 | in ≥ 40 years: 7.73% (6.89−8.67) |
| Coxofemoral osteoarthritis | 922 | 1.28% | 1284 | in ≥ 40 years: 5.13% (4.40−5.99) |
| Osteoarthritis of the knee | 2587 | 3.60% | 3604 | in ≥ 40 years: 13.83% (12.66−15.11) |
| Generalised osteoarthritis | 1105 | 1.54% | 1539 | |
| Other locations | 3394 | 4.73% | 4728 | |
| Rheumatisms of soft tissues | 7199 | 10.03% | 10,029 | |
| Fibromyalgia | 976 | 1.36% | 1360 | 2.45 (2.06−2.90) |
| Chronic back pain (including osteoarthritis) | 13,656 | 19.0% | 19,023 | |
| Cervical osteoarthritis | 846 | 1.18% | 1179 | |
| lumbar osteoarthritis | 2843 | 3.96% | 3960 | In ≥ 40 years: 10.10 (9.07−11.24) |
| Chronic cervical pain | 5125 | 7.14% | 7139 | In ≥ 40 years: 15.52 (14.30−16.83) |
| Chronic lumbar pain | 11,141 | 15.2% | 15,520 | |
| Osteoporosis | 2913 | 4.06% | 4058 | Osteoporotic fracture In ≥ 40 years: 1.83 (1.41−2.37) |
| Connective tissue diseases | 213 | .30% | 297 | |
| Systemic lupus erythmatosus | 93 | .13% | 130 | .21% (.11−.40) |
| Sjögren’s syndrome | 84 | .12% | 117 | .33% (.21−.53) |
| Scleroderma | 19 | .03% | 26 | |
| Others | 17 | .02% | 24 | |
| Myopathis | 14 | .02% | 20 | |
| Vasculitis | 66 | .09% | 92 | |
| Anti-neutrophil cytoplasmic antibody-associated vasculitis (ANCA) | 5 | .01% | 7 | |
| Non-ANCA vasculitis | 61 | .08% | 85 | |
| Others | ||||
| Rheumatic polymyalgia | 284 | .40% | 396 | |
| Undifferentiated monoarthritis | 110 | .15% | 153 | |
Data are expressed as a number, percentage and cases per 100,000 inhabitants. Comparative data obtained in the 2016 EPISER4,5 are included.
The prevalence of rheumatic disease detected in our analysis from administrative databases is 36.2%. Prevalence studies of different rheumatic diseases in the general population are usually carried out by means of surveys or questionnaires with a representative sample of the population studied. The strategies used for screening can be diverse, such as telephone surveys,16–19 face-to-face surveys12–22 or mailings,23,24 which in some cases are supplemented with clinical information to confirm the results. Among this type of study is the EPISER 2016 study, conducted on a random sample of 4916 adults representative of the Spanish population, and with a detected prevalence of 28.9 (95% CI 27.6–30.2),4,5 although the set of diagnoses evaluated in this case is lower than in our study.
In the 2016 EPISER study the lack of published data based on global results of consultations for osteoarticular pathology in primary care, emergency and hospital care was flagged up.3 Our study responds to this gap by assessing the prevalence of different rheumatic diseases in a population of 71,785 adults, using routine care coding records. This methodology makes it possible to obtain a complete picture that can only be applied when there is a system with unified information from all the healthcare facilities in a specific territory, with activity and coding records, as is the case of SSIBE.
We compared the prevalences obtained in our population with the results of the EPISER 2016 population-based study4,5 (Table 2) and observed different behaviours according to the disease analysed. The prevalence of rheumatoid arthritis (0.68%) and systemic lupus erythematosus (.13%) is within the expected results (lower confidence interval described in EPISER). In the case of ankylosing spondylitis (<-- -->0.4%), the prevalence is almost double that described in EPISER (.26%), but also within the confidence interval. The prevalences we detected are clearly lower in psoriatic arthritis, gout, fibromyalgia and Sjögren's syndrome. These differences in prevalence may be due to the different methodologies used or to errors in them, without being able to rule out that there are real territorial differences within the same country, although this has not been demonstrated.
In other diseases analysed, comparison is not possible because different inclusion criteria have been used. For example, the prevalence of osteoarthritis in our population as a whole (3.6% for knee osteoarthritis and 1.3% for coxofemoral osteoarthritis) is not directly comparable with the EPISER 2016 data, which only include adults over 40 years of age with symptomatic osteoarthritis. In osteoporosis, direct comparison is not possible either, given that we assessed the existence of this diagnosis and EPISER analysed the presence of osteoporotic fracture in those over 40 years of age. Our data also differ in vertebral, lumbar and cervical osteoarthritis, as EPISER assesses the existence of these two diagnoses and in our case a distinction is made, for both locations, between a diagnosis of osteoarthritis or simply the existence of lumbar or cervical pain (which may or may not be related to osteoarthritis).
Another benchmark population-based study was carried out by the Sisó-Almirall group in Catalonia during the period 2012−17,25 which analysed the prevalence of 78 autoimmune, systemic and organ-specific diseases in the population of Catalonia using the data analysis programme for research and innovation in health (MASCAT-PADRIS Big Data Project). This programme uses the clinical dataset reported in the integrated public health system of Catalonia through the minimum basic datasets of different care areas. The data generated from the ICD-9-CM coding is used, although in the years analysed the coding from hospital outpatient clinics (where rheumatic diseases are mainly treated) was not fully included. During this period, 779,003 people (10.6% prevalence) were detected with one of the diagnoses analysed. Although the data are not strictly comparable to ours, given that the age of the population was not limited and the period analysed was 5 years, some results are worth highlighting. These authors describe the prevalence of the different diseases per 100,000 inhabitants with the following results: adult rheumatoid arthritis (553 vs. 680 in our study), ankylosing spondylitis (137 vs. 396) and psoriatic arthropathy (57 vs. 311). These figures are all lower than ours, especially the spondyloarthropathies. The prevalence of polymyalgia rheumatica is practically the same as ours (401 vs. 396). In contrast, the prevalence of other diseases such as systemic lupus erythematosus (158 vs. 130) or Sjögren's syndrome (260 vs. 117) are clearly higher than those observed in our analysis. No comparison can be made for diseases such as vasculitis or scleroderma due to the low case rate in our series. The differences with our results are probably a consequence of several variables; the populations studied may have different characteristics between our regional population and the rest of the overall population of Catalonia and, in addition, the fact of having data from a specialised rheumatology clinic allows for better detection and recording of diseases specific to this speciality such as rheumatoid arthritis or spondyloarthritis. Nor can a bias be ruled out, especially for the more complex systemic diseases, in the type of hospital in which the activity carried out is assessed, in our case a basic general hospital and in MASCAT-PADRIS all hospitals, including those of greater complexity.
In our study, the risk of suffering from rheumatic diseases among women is 1.33, which represents an increase of 15% of women affected in the rheumatic disease group. This is consistent with the data provided in the Women and Health Report 2008–2009, which states that in Spain, women are 1.8 times more likely than men to have a chronic problem, and 1.5 times more likely to have their activity limited as a result, regardless of their age, social class, cultural level or employment status.26
The most common musculoskeletal diseases in women (osteoarthritis, arthrosis and osteoporosis) increase with age and are more common between the ages of 45–64 years.26 Back pain (cervical and lumbar) also increases with age, with a high prevalence already in the 30–44 age group, and is one of the most frequent chronic problems in women aged 16–29 years.26 In our study, the mean age of women with rheumatic disease was 60.1 years, slightly higher than that of men (57.6 years).
Epidemiological studies based on surveys with a good design and appropriate methodology allow for results that are representative of the population studied; but on the other hand, they have a high cost and the possibility of error due to the self-referential component of the data. The main limitation of studies based on administrative data is that the accuracy of coding by professionals determines the quality of the results obtained, but they do not have a special added cost and, as they analyse a whole population and not a sample, the results are not estimates but exact measurements. However, the results correspond to a specific geographical area, with certain characteristics of the population, such as population pyramid or socio-economic level, which may not coincide and therefore may not be representative of a wider population, in this case Spain.
Our work has high internal validity, but external validity needs to be tested. Our comparison with the EPISER 2016 and MASCAT-PADRIS studies highlights the similarities and differences, without being able to reach definitive conclusions. They only allow us to establish that the methodology used in this study can be applied and therefore it would be desirable to carry out other similar studies that would allow comparison between different areas of Spain and/or other countries. In this sense, the information extracted from these comparisons could be used to correct any coding errors detected and to narrow down the inclusion criteria used in the same way. Similarly, more selective and disease-specific studies would allow validation of the results obtained from administrative databases, which are more recently referred to as real-world data. Notwithstanding, the data provided contribute to increasing knowledge on the prevalence of rheumatological diseases in our environment.
Conclusions36.2% of the Baix Empordà population has some type of rheumatic disease. The estimated prevalence of different diseases partially coincides with that estimated by the EPISER 2016 study. Rheumatic disease affects a greater proportion of women, and is more frequent in patients between 55 and 75 years of age.
It is possible to identify the population presenting with rheumatic diseases by using administrative databases that collect the systematic coding of episodes of care from all levels of care.
FinancingThe study was directly funded by the Societat Catalana de Reumatologia.
The medical writer of this manuscript was funded by AbbVie under a service contract. AbbVie did not select authors to participate in the manuscript. No payment was made to the authors for the development of this manuscript.
The authors retained full control over the content of the manuscript, and the manuscript reflects their views. AbbVie did not review the final draft of the manuscript for scientific accuracy, and was not involved in the methodology, data collection and analysis, or editing
Conflict of interestsThe authors have no conflict of interests to declare.
The following is Supplementary data to this article:

Please cite this article as: Larrosa Padró M, Inoriza JM, Valls García R, Armengol Pérez E, Nolla JM, Coderch de Lassaletta J, et al. Prevalencia de las enfermedades reumáticas en el Baix Empordà. Reumatol Clín. 2022;18:551–556.


