


The status of private rheumatology is known, but there is no information on the kind of patients seen. This study describes the experience over a 3-year period in a private rheumatology practice in the Autonomous Community of Madrid. We collected demographic and descriptive data. Of 706 patients seen, almost half (46%) were there for their first visit, and 12% of patients who had asked for an appointment did not attend. The majority of patients were women (72.4%) with a median age of 44.3 years old (range 3–93). The most frequent diagnoses were osteoarthritis (20.9%), osteopenia/osteoporosis (16.8%), arthralgia (13.4%) and soft tissue disorder (9.6%). The majority of the patients had private insurance with Spanish companies, such as MAPFRE, Adeslas and Asisa. At least one quarter of ancillary tests ordered in the first visit were not revised on a second visit.
Se conoce el estado de la reumatología privada en España, pero no hay información sobre el tipo de pacientes atendidos. Este estudio describe la experiencia de varios años de práctica de reumatología privada a tiempo parcial en la comunidad autónoma de Madrid. Se recogieron los datos demográficos y descriptivos de consulta de pacientes atendidos de forma consecutiva durante 3 años. De un total de 706 pacientes atendidos, casi la mitad (46%) solo acudió una vez a consulta y el 12% de los pacientes que se citaron no llegaron a presentarse a la cita. La mayor parte de los pacientes fueron mujeres (72,4%) con una edad media de 44,3 años (rango 3-93). Los diagnósticos más frecuentes fueron artrosis (20,9%), osteopenia/osteoporosis (16,8%), artromialgias inespecíficas (13,4%) y reumatismos de partes blandas (9,6%). La mayoría de los pacientes, un 83,1% (587 pacientes), eran clientes de las compañías MAPFRE, Adeslas y Asisa. Aproximadamente una cuarta parte de las pruebas complementarias que se piden en consulta no se revisan en consultas posteriores.
This musculoskeletal disease is very common in the general population, generating 20% of primary care consultations.1 The epidemiological study by the Spanish Society of Rheumatology at the end of the 90s showed that over 20% of people over 20 presented with some type of rheumatologic disease.2 Consultations in this area in private medicine is divided between trauma, rehabilitation and rheumatology specialties.
Private rheumatology is a speciality area which has boomed in recent years, 38.2% of Spanish rheumatologists practise the specialty in the private sector, the majority of them in mixed form (25%).3 The autonomous communities with the greatest number of rheumatologists who practise privately are Catalonia and Madrid.3 The private sector is highly relevant, since approximately a third of the national health budget was dedicated to private medicine in 20132 and specifically over 700 million euros in the autonomous community of Madrid (CAM).3
We are currently aware of the state of private rheumatology in Spain related to professionals and distribution by autonomous communities,4 but no information exists regarding the type of patient and the diseases they deal with. The CAM has 150 rheumatologists on public hospital staffs 33.8% of whom also work in the private sector.5 No precise details exist regarding the number of rheumatologists who exclusively practise in the private sector today, but the Spanish Society of Rheumatology is currently making attempts to rectify this.
In general, it is accepted that the diseases attended in rheumatology in the private sector and in the public sector are similar, where over 25% of care is dedicated to inflammatory disease, whilst osteoarthritis and osteoporosis make up a slightly lower percentage (21%), but certain differences may exist.6 Lamentably, there is little available information relating to private practice. Knowledge regarding patient type and disease diagnosed, together with resources consumed, is important for better management and quality in private rheumatology practice, being beneficial both for the national health system, for the rheumatologists and above all for the patient.1
The aim of this descriptive study of private outpatient rheumatology practise is to provide information on the disease and the general traits of the patients cared for.
PatientsAn observational descriptive study of patients who were consecutively seen in 2 private rheumatology medical centres for 3 years. This included patients who were attended in the Hospital Ruber Internacional and in the Armstrong Clinic, both in Madrid. In both centres, outpatient care was undertaken in external consultancy once a week, with the possibility of hospital admittance. Consultations from emergencies and day hospital only took place in the Hospital Ruber Internacional. Ultrasound scans were not available in either of the 2 centres, which depended on X-ray services for imaging technique, whilst the capillaroscopy was available only in the Hospital Ruber Internacional.
Demographic data was collected (age, gender, date of first consultation and diagnosis) and descriptive data from the private practice (insurance company or private company, total number of appointments, new consultations vs check-up, number of consultations not presented, tests requested and interconsultations to other specialists). The patients freely requested consultation. New consultations were considered to be all those patients who were attended for the first time and check-ups were all subsequent consultations. A non attended consultation was that where an appointment was requested and the patient did not present, but did not previously cancel the appointment.
The initial diagnostic impression or the final diagnosis, whenever possible, were collected and were summarised as chronic arthritis (rheumatoid arthritis, spondyloartritis, psoriatic arthritis, idiopathic juvenile arthritis, connective tissue diseases (lupus, inflammatory myopathies, Sjögren's syndrome and scleroderma), osteopenia/osteoporosis, osteoarthritis (regardless of location), non specific arthromyalgias, soft tissue rheumatisms (e.g. epichondylitis, trochanteritis, mechanical plantar fasciitis, etc.), microcrystalline arthritis (gouty arthritis and calcium pyrophosphate dehydrate arthritis), non-specific axial pain (non inflammatory lumbago, back pain and cervical pain), analytical alterations (positive antibodies, increase in acute phase reactants or muscle enzymes, raised anti-strepomycin antibodies, etc.), fibromyalgia, rheumatic polymyalgia and “others”. Included in “others” are those diseases which make up under 1% of the total patients attended (e.g. episcleritis, idiopathic hyperostosis, Raynaud's phenomenon, Paget's disease, etc.).
Further tests were requested, blood sample and imaging tests (plain X-rays, musculoskeletal ultrasound (MSU), densitometries, magnetic resonances [MR] and computerised tomographies), together with interconsultations with other specialities.
The results are presented in total numbers and percentages (%) for the qualitative variables and in medians and range for the qualitative variables.
Results706 patients were attended in 207 days of consultation, with a mean of 7.2 patients seen per day. A total of 1493 medical visits were programmed, there were 706 (47.3%) new consultations and 612 (41%) check-ups, whilst consultations which patients did not attend were 175 (11.7%). Median age was 44.3 years (range 3–93) and 511 patients were women (72.4%). The majority of patients, 83.1% (587 patients), were clients of the companies MAPFRE, Adeslas and Asisa. The complete list of patients, and which insurance companies they belonged to is shown in Fig. 1.

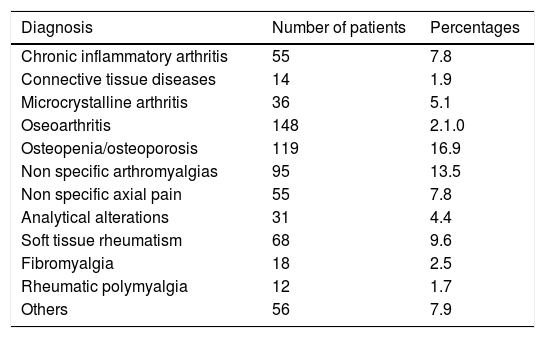
The most common diagnoses were osteoarthritis (148 patients, 20.9%), osteopenia/osteoporosis (119 patients, 16.8%), non specific arthromyalgias (95 patients, 13.4%) and the soft tissue rheumatisms (68 patients, 9.6%). The first three diagnoses made up for 51% of patients and together with rheumatisms of soft tissues they covered 61% of total diagnoses. The complete list of diagnoses is presented in Table 1.
Diagnostic Impression or Final Diagnoses of the Patients Seen in the Private Outpatients Department.
| Diagnosis | Number of patients | Percentages |
|---|---|---|
| Chronic inflammatory arthritis | 55 | 7.8 |
| Connective tissue diseases | 14 | 1.9 |
| Microcrystalline arthritis | 36 | 5.1 |
| Oseoarthritis | 148 | 2.1.0 |
| Osteopenia/osteoporosis | 119 | 16.9 |
| Non specific arthromyalgias | 95 | 13.5 |
| Non specific axial pain | 55 | 7.8 |
| Analytical alterations | 31 | 4.4 |
| Soft tissue rheumatism | 68 | 9.6 |
| Fibromyalgia | 18 | 2.5 |
| Rheumatic polymyalgia | 12 | 1.7 |
| Others | 56 | 7.9 |
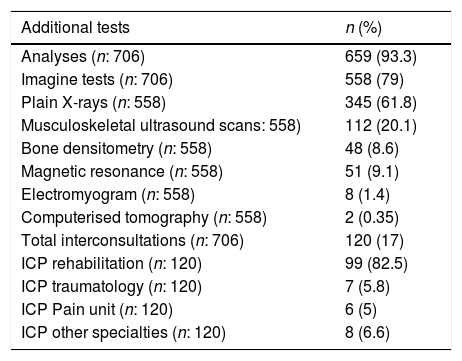
A total of 659 analytic tests were requested (0.5 per visit) and 558 imaging tests (0.42 per visit). Of the imaging tests, plain X-ray was the most frequent, 61.8% (345 X-rays), MSU was 20.1% (112), MR 9.1% (51) and densitometries 8.6% (48); only 2 tomographies were requested. 120 interconsultations were requested from other specialities, 99 (82.5%) from the rehabilitation service. The other interconsultations were divided into 7 (5.8%) from traumatology, 6 (5%) from the pain unit, 2 (1.6%) from the digestive and endocrinology unit and one interconsultation (0.8%) from dermatology, immunology, ophthalmology and pneumology. The total list of complementary tests and interconsultations is contained in Table 2.
List of Additional Tests and Interconsultations Requested in the Private Outpatients Consultation.
| Additional tests | n (%) |
|---|---|
| Analyses (n: 706) | 659 (93.3) |
| Imagine tests (n: 706) | 558 (79) |
| Plain X-rays (n: 558) | 345 (61.8) |
| Musculoskeletal ultrasound scans: 558) | 112 (20.1) |
| Bone densitometry (n: 558) | 48 (8.6) |
| Magnetic resonance (n: 558) | 51 (9.1) |
| Electromyogram (n: 558) | 8 (1.4) |
| Computerised tomography (n: 558) | 2 (0.35) |
| Total interconsultations (n: 706) | 120 (17) |
| ICP rehabilitation (n: 120) | 99 (82.5) |
| ICP traumatology (n: 120) | 7 (5.8) |
| ICP Pain unit (n: 120) | 6 (5) |
| ICP other specialties (n: 120) | 8 (6.6) |
Out of the total patients 325 (46%) were attended just once. Of the 381 patients who went at least once for a check-up, mean time of follow-up was 1.3 years (range 0 to 3 years). In that initial consultation 155 analytical tests were requested, 173 imaging tests and 32 interconsultations (30 from rehabilitation). As a consequence, the result of 23.5% of the analyses and 27.6% of the imaging tests requested during the initial consultation were not reviewed in a second consultation. Imaging tests made up for 20.8% of densitometries (10/48), 29.4% of MR (15/51), 21.4% of MSU (24/112) and 30.1% of plain X-rays (104/345). Demographic characteristics and the percentage of different diagnoses in this subgroup of patients was super-imposable with the total patients.
DiscussionDuring the 3 years of private rheumatology practice, mostly middle aged women who had an insurance policy were seen. They presented with osteoarthritis, osteoporosis, non specific arthromyalgias or soft tissue rheumatisms. The situation of rheumatology in public medicine has been studied on a national level and autonomous community level4,6–8 and also recently in private healthcare,3 but there is still very little information relating to the high percentage of patients who are seen by private rheumatology departments. In our study, care of osteoarthritis and osteoporosis account for 38% of the work load, whilst chronic arthritis accounts for 7,8% and connective tissue diseases for 1.9%. The study by Lázaro et al., undertaken in the CAM in 2013, described that in public rheumatology services chronic arthritis accounted for almost 30% of the work load and connective tissue diseases for 9.4%; but osteoarthritis and osteoporosis accounted for 21% of it.5 There are therefore differences in the diseases attended by private rheumatology departments (more osteoarthritis and osteoporosis) and public ones (more chronic arthritis and connective tissue diseases). Notwithstanding, further studies are needed to confirm these differences.
In our study, approximately one out of every 10 patients who requested consultation in private rheumatology departments did not attend their consultation, and had no scientific literature with which to compare these results with the public medical sector. Of particular interest was the fact that almost half of the patients (46%) with appointments in the private sector were only seen once and that one out of every 4 tests requested, or analytical test and imaging tests were not reviewed in a second consultation. It is not possible to know whether they were reviewed by other specialities or were not undertaken, but maybe the initial consultation resolved the doubts for many patients about whether the pain they presented with was due to a serious illness and they did not complete the additional tests requested.
In contrast to the general concept of private medicine, the number of patients seen privately is a low percentage (3%), with the majority of patients (>80%) being clients of the main insurance companies (MAPFRE, Adeslas and Asisa). Our results may not of course be extrapolated totally to CAM, due to the number of patients seen and also that despite the great majority being available, some of the existing insurers were not available in any of the 2 centres where the study was carried out.
The additional tests most requested were analyses and imaging tests (X-rays, MSU and MR), one for each 2 consultations, and the most interconsulted specialty was rehabilitation (>82% of interconsultations). The availability of an ultrasound in private rheumatology consultation facilitates diagnosis and the resolution of many soft tissue processes seen, reducing the number of check-ups and interconsultations to rehabilitation, as well as reducing the number of imaging studies, and in particular those of extra MSU and MR studies.
The main limitation of this study is its limited external validity with information on 2 private rheumatology centres of the CAM being provided, and with the need for further studies (with the inclusion of care quality or severity of patients seen) and multicentres to confirm these findings. Furthermore, the general descriptive nature of the study and the coding of the diagnoses, without making use of code CIE-9 could be a limiting study factor. However, for the most part the diseases seen are highly prevalent and well differentiated from one another.
To conclude, private outpatient rheumatology in the CAM mainly treats middle-aged women with an insurance policy who present with osteoarthritis, osteoporosis, non-specific arthromyalgias or soft tissue rheumatisms. However, a quarter of the imaging studies and analyses requested were not undertaken or reviewed by the specialist who requested them.
Conflict of InterestsThe author confirms that there are no conflicts of interest in this document.
To all patients who requested an appointment with me over recent years, for their trust and experience.
Please cite this article as: Nieto González JC. Reumatología privada ambulatoria, estudio descriptivo en la Comunidad de Madrid. Reumatol Clin. 2019;15:e10–e13.


