

Behçet's disease(BD) is a systemic vasculitis which may affect the quality of life (QoL).
AimsThis study aimed to assess the QoL in Iranian Azeri BD patients as well as evaluating the association between QoL and disease characteristics including disease activity and clinical symptoms.
MethodsIn this cross-sectional study, a total of 123 BD patients aged 15–65 years fulfilling International Criteria for BD and 123 healthy controls matched with regard to gender were included. Patients aged 15–18 years had the informed consent and consent of their parents for participation. Short Form-36 Quality of Life Scale (SF-36) was used to evaluate QoL. Disease activity was measured by Behcet's Disease Current Activity Form and the Iranian Behcet's Disease Dynamic Activity Measure and Vasculitis Damage Index (VDI) was used for the clinical assessment of damage.
ResultsThe mean±SD age of BD patients and control group was 38.19±10.99 and 33.65±7.29 years, respectively. The Physical Health score as well as most of SF-36 domains including Role Physical, Bodily Pain, General Health, Vitality, and Mental Health were significantly lower in BD patients compared with the control group (P<0.05). There was significant correlation between the Physical and Mental Health scores and most of SF-36 domains with disease activity and clinical symptoms including genital ulcers, ophthalmic and central nervous system (CNS) involvement (P<0.05). Significant correlation was only observed between VDI and Bodily Pain domain (P<0.05).
ConclusionQuality of life is impaired in BD patients, and this impairment is related with disease severity. It seems that presence of genital ulcers, eye and CNS involvement lead to the impairment of QoL in BD patients. These results highlight the importance of nursing interventions in managing clinical symptoms in these patients.
La enfermedad de Behçet (BD) es una vasculitis sistémica que puede afectar la calidad de vida (QoL).
ObjetivosEste estudio tuvo como objetivo evaluar la QoL en pacientes con BD azerí iraní, así como evaluar la asociación entre la QoL y las características de la enfermedad, incluida la actividad de la enfermedad y los síntomas clínicos.
MétodosEn este estudio transversal, un total de 123 pacientes con BD de 15 a 65 años de edad cumplieron con los criterios internacionales para BD y 123 controles sanos que fueron emparejados por género. Los pacientes de 15 a 18 años de edad tenían el consentimiento informado y el consentimiento de sus padres para participar en el estudio. Se usó la escala de calidad de vida corta-36 (SF-36) para evaluar la calidad de vida. La actividad de la enfermedad se midió mediante el formulario de actividad actual de la BD y la medida de la actividad dinámica de la BD iraní y el índice de daño de la vasculitis (VDI) se usaron para la evaluación clínica del daño.
ResultadosLa media±DE de los pacientes con BD y el grupo control fue de 38,19±10,99 y 33,65±7,29 años, respectivamente. La puntuación de Salud física, así como la mayoría de los dominios SF-36, incluyendo Rol físico, Dolor corporal, Salud general, Vitalidad y Salud mental, fueron significativamente más bajos en los pacientes con BD en comparación con el grupo control (p<0,05). Hubo una correlación significativa entre los puntajes de Salud física y mental y la mayoría de los dominios SF-36 con actividad de la enfermedad y síntomas clínicos, como úlceras genitales, compromiso del sistema oftálmico y del sistema nervioso central (SNC) (p<0,05). Solo se observó una correlación significativa entre el VDI y el dominio del dolor corporal (p<0,05).
ConclusiónLa calidad de vida se ve afectada en los pacientes con BD, y este deterioro está relacionado con la gravedad de la enfermedad. Parece que la presencia de las úlceras genitales, la afectación ocular y del SNC conduce al deterioro de la QoL en pacientes con BD. Estos resultados resaltan la importancia de las intervenciones de enfermería en el manejo de los síntomas clínicos en estos pacientes.
Behçet's disease is one of the rheumatologic disorders related to vasculitis which affects most commonly young adults.1 It is more prevalent in Mediterranean countries such as Turkey, Greece, Israel; Middle Eastern countries such as Iraq and Iran as well as Far Eastern countries such as Japan, Korea, and China.2,3 Common symptoms include oral and genital ulcers, skin lesions and arthritis, which might be accompanied by ocular and vascular involvements.4 These symptoms not only have negative effect on physical and mental health of patients, but they also diminish their quality of life (QoL) by causing several physical impairments.5
The QoL becomes as an important outcome variable in patients with chronic diseases. Measurement of Health-Related Quality of Life (HRQoL) plays an important role in treatment decisions and assessing the course of the disease. QoL is a concept that includes being able to satisfy one's own basic needs, being satisfied with life, showing enough social interaction, allocating time to fun, feeling good emotionally and physically, being good at interpersonal relationships, having self-esteem as well as previous experiences. Therefore, it could be defined as perception of people about life, values, goals, standards, and interests. Recent studies indicated that QoL in patients with Behçet disease was negatively affected by the disease.6–13 According to previous investigations, there is a stress factor in most patients with BD before the initial onset or relapse of the disease.14–16 Furthermore, it has been reported that subjects with BD have higher anxiety and depression levels14,15 and lower quality of life (QoL) than healthy controls.7,12
QoL evaluation could help in developing more detailed care plans that ensure a better understanding of the behaviors and the psychological reactions of the patients as well as the difficulties they experience with adjusting to the disease and developing effective coping mechanisms.17 Since BD is a chronic disease having a relapsing course therefore, complaints associated with BD have adverse effects on physical and mental health and attenuates QoL by generating certain physical problems.6
Short-Form-36 (SF-36) is the most commonly used international scale and is considered a valid instrument for measuring physical functioning and comparing different aspects of health related QoL in patients with rheumatologic diseases.18 To the best of our knowledge, there is no study evaluating QoL in Iranian Azeri Behçet patients using SF-36, therefore this study aimed to assess the QoL in this population as well as evaluating the association between QoL and disease characteristics including disease activity and clinical symptoms.
Materials and methodsStudy design and participantsIn this cross-sectional study conducted in Tabriz, the North-West of Iran, a total of 123 BD patients aged 15–65 years fulfilling International Criteria for Behcet's Disease19,20 were recruited from the rheumatology outpatient clinic of Tabriz University of Medical Sciences. The control group included 123 healthy subjects who were matched with regard to gender. Individuals with chronic inflammatory and/or degenerative diseases were excluded from the study.
The study protocol was approved by the Ethics Committee of Tabriz University of Medical Sciences (Iran) and performed according to the Helsinki humanity research declaration (2008). Written informed consent was obtained from all subjects before participating in the study. Patients aged 15–18 years had the informed consent and consent of their parents for participation. During the study, all the personal information was kept confidential and other ethical and considerations of humanity were performed as well.
Evaluation of quality of lifeShort Form-36 Quality of Life Scale (SF-36 QoL Scale) was used to evaluate quality of life. SF-36 is a scale for quality of life consists of the following 8 subcategories: (a) Physical Functioning (10 items), (b) Social Functioning (2 items), (c) Role Physical (4 items), (d) Role Emotional (3 items), (e) Mental Health (5 items), (f) Vitality (4 items), (g) Bodily Pain (2 items), (h) General Health (5 items). The scale was evaluated taking the last 4 weeks into account. All items except the third and fourth were rated on a Likert scale. The third and fourth items were yes or no questions. The scores assigned to each category ranged from 0 to 100, where 0 and 100 represented the lowest and highest QoL, respectively.21 This scale was translated into Persian and assessed for validity and reliability by Montazeri et al.22 The Iranian version of the SF-36 performed well and the results indicated that it was a reliable and valid measure of health related quality of life. The internal consistency (to test reliability) showed that all eight SF-36 scales met the minimum reliability standard, the Cronbach's α coefficients ranging from 0.77 to 0.90 with the exception of the vitality scale (α=0.65). Known groups comparison (to test validity) showed that in all scales the SF-36 discriminated between men and women, and old and the young respondents as anticipated (all P values<0.05). Convergent validity (to test scaling assumptions) using each item correlation with its hypothesized scale showed satisfactory results (all correlation above 0.40 ranging from 0.58 to 0.95). Also, factor analysis identified two principal components that jointly accounted for 65.9% of the variance.22
Clinical assessmentDisease activity was measured by Behcet's Disease Current Activity Form (BDCAF) and the Iranian Behcet's Disease Dynamic Activity Measure (IBDDAM).23,24 In order to calculate IBDDAM, points were given to the non-ophthalmic manifestations of BD according to its severity and duration and total scores are between 0 and 32. Furthermore, Vasculitis Damage Index (VDI)25 was used for the clinical assessment of damage in BD patients.
Statistical analysisStatistical analyses were conducted using the SPSS statistical package (SPSS Inc., version 16). The normality of data was tested by Kolmogorov–Smirnov test. Independent sample t-test for continuous variables and chi-square test for categorical variables were used to determine differences between two groups. Correlations between variables were determined by Spearman correlation analysis. P-values<0.05 were considered statistically significant.
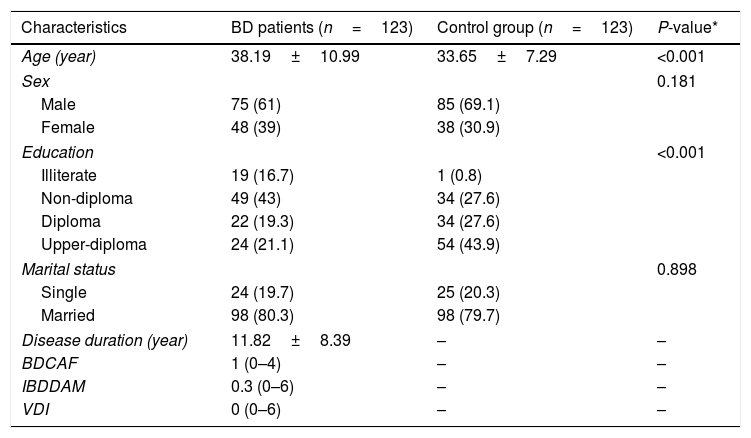
ResultsTable 1 presents baseline characteristics of BD patients and controls. The mean±SD age of BD patients and control group was 38.19±10.99 (Min–Max: 15–62) and 33.65±7.29 (Min–Max: 17–58) years, respectively. Sixty-one percent of patients and 69.1% of control group were males. Mean duration of disease in BD patients was 11.82±8.39 years and the median (Min–Max) of BDCAF, IBDDAM and VDI were 1 (0–4), 0.3 (0–6) and 0 (0–6), respectively. There was significant difference in mean age and education level between the two groups (P<0.05); whilst no significant difference was observed in gender and marital status between the two groups (P>0.05).
Baseline characteristics of BD patients and controls.
| Characteristics | BD patients (n=123) | Control group (n=123) | P-value* |
|---|---|---|---|
| Age (year) | 38.19±10.99 | 33.65±7.29 | <0.001 |
| Sex | 0.181 | ||
| Male | 75 (61) | 85 (69.1) | |
| Female | 48 (39) | 38 (30.9) | |
| Education | <0.001 | ||
| Illiterate | 19 (16.7) | 1 (0.8) | |
| Non-diploma | 49 (43) | 34 (27.6) | |
| Diploma | 22 (19.3) | 34 (27.6) | |
| Upper-diploma | 24 (21.1) | 54 (43.9) | |
| Marital status | 0.898 | ||
| Single | 24 (19.7) | 25 (20.3) | |
| Married | 98 (80.3) | 98 (79.7) | |
| Disease duration (year) | 11.82±8.39 | – | – |
| BDCAF | 1 (0–4) | – | – |
| IBDDAM | 0.3 (0–6) | – | – |
| VDI | 0 (0–6) | – | – |
BDCAF: Behcet's Disease Current Activity Form; IBDDAM: Iranian Behcet's Disease Dynamic Activity Measure; VDI: Vasculitis Damage Index.
Data are presented as mean±SD, number (%) or median (Min–Max).
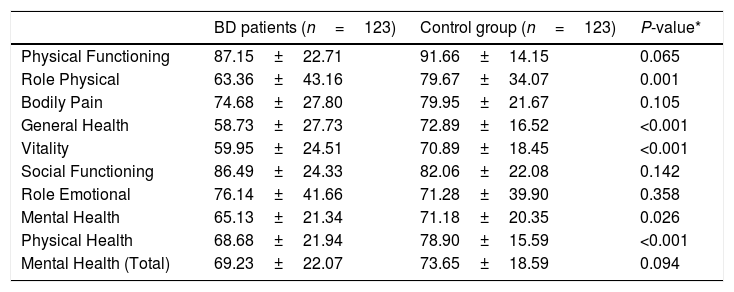
As indicated in Table 2, the Physical Health score as well as most of SF-36 domains including Role Physical, Bodily Pain, General Health, Vitality, and Mental Health were significantly lower in BD patients compared with the control group (P<0.05).
SF-36 scores of BD patients and controls.
| BD patients (n=123) | Control group (n=123) | P-value* | |
|---|---|---|---|
| Physical Functioning | 87.15±22.71 | 91.66±14.15 | 0.065 |
| Role Physical | 63.36±43.16 | 79.67±34.07 | 0.001 |
| Bodily Pain | 74.68±27.80 | 79.95±21.67 | 0.105 |
| General Health | 58.73±27.73 | 72.89±16.52 | <0.001 |
| Vitality | 59.95±24.51 | 70.89±18.45 | <0.001 |
| Social Functioning | 86.49±24.33 | 82.06±22.08 | 0.142 |
| Role Emotional | 76.14±41.66 | 71.28±39.90 | 0.358 |
| Mental Health | 65.13±21.34 | 71.18±20.35 | 0.026 |
| Physical Health | 68.68±21.94 | 78.90±15.59 | <0.001 |
| Mental Health (Total) | 69.23±22.07 | 73.65±18.59 | 0.094 |
P<0.05 was considered significant.
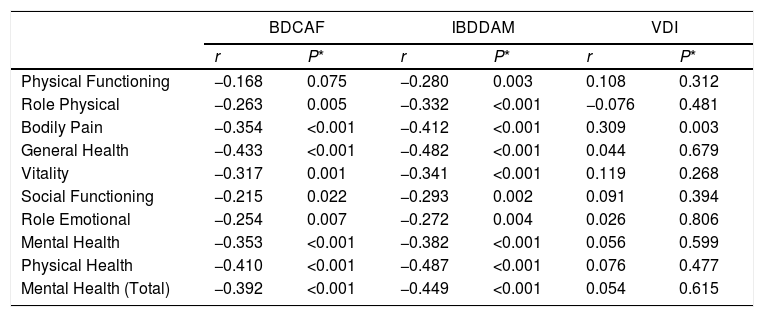
Table 3 depicts correlation between SF-36 scores with disease activity and VDI in patients with Behçet's disease. According to Table 3, there was significant correlation between the Physical and Mental Health scores and most of SF-36 domains with disease activity (P<0.05); whilst significant correlation was only observed between VDI and Bodily Pain domain (P<0.05).
Correlation between SF-36 scores with disease activity and VDI in patients with Behçet's disease (n=123).
| BDCAF | IBDDAM | VDI | ||||
|---|---|---|---|---|---|---|
| r | P* | r | P* | r | P* | |
| Physical Functioning | −0.168 | 0.075 | −0.280 | 0.003 | 0.108 | 0.312 |
| Role Physical | −0.263 | 0.005 | −0.332 | <0.001 | −0.076 | 0.481 |
| Bodily Pain | −0.354 | <0.001 | −0.412 | <0.001 | 0.309 | 0.003 |
| General Health | −0.433 | <0.001 | −0.482 | <0.001 | 0.044 | 0.679 |
| Vitality | −0.317 | 0.001 | −0.341 | <0.001 | 0.119 | 0.268 |
| Social Functioning | −0.215 | 0.022 | −0.293 | 0.002 | 0.091 | 0.394 |
| Role Emotional | −0.254 | 0.007 | −0.272 | 0.004 | 0.026 | 0.806 |
| Mental Health | −0.353 | <0.001 | −0.382 | <0.001 | 0.056 | 0.599 |
| Physical Health | −0.410 | <0.001 | −0.487 | <0.001 | 0.076 | 0.477 |
| Mental Health (Total) | −0.392 | <0.001 | −0.449 | <0.001 | 0.054 | 0.615 |
BDCAF: Behcet's Disease Current Activity Form; IBDDAM: Iranian Behcet's Disease Dynamic Activity Measure; VDI: Vasculitis Damage Index.
P<0.05 was considered significant.
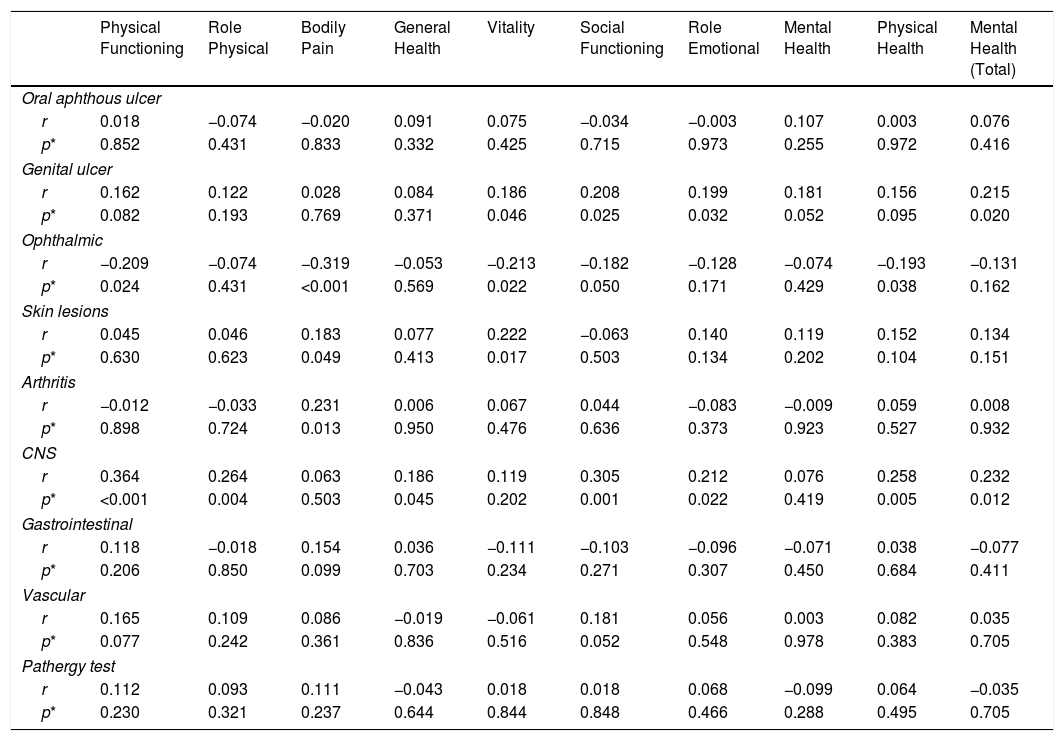
Table 4 presents correlation between SF-36 scores and clinical symptoms in patients with Behçet's disease. As indicated in Table 4, there was significant correlation between the Physical and Mental Health scores and some SF-36 domains with genital ulcers, ophthalmic and central nervous system (CNS) involvement (P<0.05). No significant correlation was observed between the Physical and Mental Health scores and some SF-36 domains with oral aphthous ulcer, skin lesions, arthritis, gastrointestinal and vascular involvement as well as pathergy test (P>0.05).
Correlation between SF-36 scores and clinical symptoms in patients with Behçet's disease (n=123).
| Physical Functioning | Role Physical | Bodily Pain | General Health | Vitality | Social Functioning | Role Emotional | Mental Health | Physical Health | Mental Health (Total) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Oral aphthous ulcer | ||||||||||
| r | 0.018 | −0.074 | −0.020 | 0.091 | 0.075 | −0.034 | −0.003 | 0.107 | 0.003 | 0.076 |
| p* | 0.852 | 0.431 | 0.833 | 0.332 | 0.425 | 0.715 | 0.973 | 0.255 | 0.972 | 0.416 |
| Genital ulcer | ||||||||||
| r | 0.162 | 0.122 | 0.028 | 0.084 | 0.186 | 0.208 | 0.199 | 0.181 | 0.156 | 0.215 |
| p* | 0.082 | 0.193 | 0.769 | 0.371 | 0.046 | 0.025 | 0.032 | 0.052 | 0.095 | 0.020 |
| Ophthalmic | ||||||||||
| r | −0.209 | −0.074 | −0.319 | −0.053 | −0.213 | −0.182 | −0.128 | −0.074 | −0.193 | −0.131 |
| p* | 0.024 | 0.431 | <0.001 | 0.569 | 0.022 | 0.050 | 0.171 | 0.429 | 0.038 | 0.162 |
| Skin lesions | ||||||||||
| r | 0.045 | 0.046 | 0.183 | 0.077 | 0.222 | −0.063 | 0.140 | 0.119 | 0.152 | 0.134 |
| p* | 0.630 | 0.623 | 0.049 | 0.413 | 0.017 | 0.503 | 0.134 | 0.202 | 0.104 | 0.151 |
| Arthritis | ||||||||||
| r | −0.012 | −0.033 | 0.231 | 0.006 | 0.067 | 0.044 | −0.083 | −0.009 | 0.059 | 0.008 |
| p* | 0.898 | 0.724 | 0.013 | 0.950 | 0.476 | 0.636 | 0.373 | 0.923 | 0.527 | 0.932 |
| CNS | ||||||||||
| r | 0.364 | 0.264 | 0.063 | 0.186 | 0.119 | 0.305 | 0.212 | 0.076 | 0.258 | 0.232 |
| p* | <0.001 | 0.004 | 0.503 | 0.045 | 0.202 | 0.001 | 0.022 | 0.419 | 0.005 | 0.012 |
| Gastrointestinal | ||||||||||
| r | 0.118 | −0.018 | 0.154 | 0.036 | −0.111 | −0.103 | −0.096 | −0.071 | 0.038 | −0.077 |
| p* | 0.206 | 0.850 | 0.099 | 0.703 | 0.234 | 0.271 | 0.307 | 0.450 | 0.684 | 0.411 |
| Vascular | ||||||||||
| r | 0.165 | 0.109 | 0.086 | −0.019 | −0.061 | 0.181 | 0.056 | 0.003 | 0.082 | 0.035 |
| p* | 0.077 | 0.242 | 0.361 | 0.836 | 0.516 | 0.052 | 0.548 | 0.978 | 0.383 | 0.705 |
| Pathergy test | ||||||||||
| r | 0.112 | 0.093 | 0.111 | −0.043 | 0.018 | 0.018 | 0.068 | −0.099 | 0.064 | −0.035 |
| p* | 0.230 | 0.321 | 0.237 | 0.644 | 0.844 | 0.848 | 0.466 | 0.288 | 0.495 | 0.705 |
CNS: Central Nervous System.
P<0.05 was considered significant.
Taking into account that BD is a chronic immunoinflammatory disease with periods of exacerbation and remission, the quality of life can be affected negatively. To the best of our knowledge, this is the first study to examine the QoL in Iranian Azeri Behçet patients. According to our study, the Physical Health score as well as most of SF-36 domains were significantly lower in BD patients, compared with the control group. Furthermore, significant correlation was observed between the Physical and Mental Health score and most of SF-36 domains with disease activity. Our findings were in agreement with the results of previous studies which showed the impaired quality of life in BD patients (6–13). Ertam et al.8 demonstrated that overall SF-36 scores as well as their domains were significantly lower in BD patients, compared with the control group. In another study, Mumcu et al.11 found that all SF-36 domains were significantly worse in BD patients than in controls. They also found that impairment in quality of life was related with disease activity in BD.11 Furthermore, Bodur et al.7 investigated the relationship between the quality of life, life satisfaction and disease activity in BD patients and compared with controls. They found that life satisfaction index scores were significantly lower and Nottingham health profile scores were significantly worse in all dimensions in BD patients. So they concluded that life satisfaction and quality were impaired in BD patients.7 Also, Canpolat et al.21 found that QoL scores in patients with Behçet's disease were low and were affected by gender, age, work status, education status as well as complaints of oral and genital ulcerations, arthritis, skin lesions and bodily pain. In another study, Tanriverdi et al.12 showed that BD patients were more susceptible to mood and anxiety disorders, and their QoL was lower than that of their healthy counterparts. They also reported that chronic diseases like BD might be related to mood disorders, which might have a negative effect on patient's daily life.
Our study also indicated significant correlation between the Physical and Mental Health scores and some SF-36 domains with genital ulcers, ophthalmic and CNS involvement. No significant correlation was observed between the Physical and Mental Health scores and some SF-36 domains with oral aphthous ulcer, skin lesions, arthritis, gastrointestinal and vascular involvement as well as pathergy test. Our findings were consistent with Tanriverdi et al.12 study which reported mental status might have triggered the development of ocular attacks in BD and that BD patients with ocular involvement had significantly more susceptibility to anxiety and depression. Similarly, Ertam et al.8 found significantly lower scores in “Mental Health” domain of SF-36 scale in BD patients with eye involvement. Moreover, the negative effect of the genital ulcers on the quality of life in BD was shown by Blackford et al.26 In other previous study, Bodur et al.7 reported that arthritis, fatigue and genital ulcer scores of BDCAF were the most important factors impairing the quality of life in BD. In contrast with present study, Gur et al.9 reported that arthritis had a negative effect on the quality of life in BD patients. Taner et al.27 used Beck depression and Beck anxiety inventory in BD patients and psoriasis patients. Although the psoriatic skin lesions might be expected to deteriorate the quality of life considerably, they reported that the quality of life of BD patients were even worse than that of the psoriasis patients. Furthermore, Ertam et al.8 indicated that presence of vascular involvement, eye involvement and arthritis contributed considerably to impaired quality of life in BD. However, they could not show that genital ulcers impaired the quality of life in BD. According to Kilinç et al.,28 patients with oral ulcer, genital ulcer, lesions that looks like erythema nodosum and gastrointestinal ulcer had lower emotional life, daily activity, symptom and sexual life scores. This discrepancy between our results with previous studies might be due to differences in studied population.
Limitations and strengthsThe limitation of the current study was that although significant correlations were observed between SF-36 scores with disease activity and some clinical symptoms, the correlations were low to moderate. The strengths of present study included the relatively large sample size and that we had a control group and compared QoL between patients with BD and normal population. Furthermore, all study subjects had a high cooperation in this research.
ConclusionIn conclusion, based on evaluation of SF-36 scores, quality of life is impaired in BD, and this impairment is related with disease severity. Presence of arthritis, eye involvement and vascular involvement seem to contribute the impairment of quality of life in BD. These results highlight the importance of nursing interventions in managing the symptoms experienced by patients effectively so that the limited effects of the symptoms which decrease QoL can be eliminated.
FundingThis study was supported by Connective Tissue Diseases Research Center of Tabriz University of Medical Sciences, Tabriz, Iran.
Conflict of interestsThe authors declare that there is no conflict of interests.
The authors wish to thank all subjects for their participation in this research.


