

We have closely read the article published by Isasi et al.1 in Reumatologia Clínica presenting a case of fibromyalgia (FM) and chronic fatigue syndrome (CFS) caused by non-celiac sensitivity to gluten (NGCD). We would like to comment our experience with this attractive topic regarding patients with FM/CFS, which I hope will contribute to an improved knowledge of this association. The authors have reasonably ruled out celiac disease (CD) and have hypothesized that NGCD is the cause of FM and CFS in their patient; upon complete remission (CR) of symptoms, both digestive and musculoskeletal, with a gluten-free diet (GFD). CFS is characterized by intense fatigue in addition to cognitive, autonomic, neurroendocrine, immunoallergic and musculoskeletal symptoms, newly appearing and inexplicable, lasting for at least 6 months. In the criteria (C) from the most recent international consensus in 2011, gastrointestinal alterations were included (irritable bowel syndrome [IBS] as was sensitivity to foodstuff) as diagnostic criteria for CFS.2 This new classification allows us to consider NGCD as a comorbid condition (CC), which perpetuates CFS and not unleashes it. In our series of 200 patients affected by CFS attended at the Unidad del Camp de Tarragona (2011–2013), we found the following CC: 101 patients (50.5%) with FM, 38 patients (19%) with chronic autoimmune thyroiditis, 31 patients (15.5%) with NGCD and 27 patients (13.5%) with IBS. At the onset of GFD, in addition to multidisciplinary treatment, most of our patients (up to 80%) had improvement of their intestinal symptoms (abdominal pain, diarrhea, flatulence, oral ulcers) and a very modest response to extra intestinal symptoms (fatigue, bone pain, alterations in concentration and depression) without reaching CR. Therefore, we have supported the theory of overlap between FM/CFS and NGCD without concluding that the latter is its cause in this patient population, but may aggravate its symptoms. This term was probably employed for the first time in 1978 by Ellis and Linaker. There is increasing evidence suggesting the existence of NGCD. This concept groups patients who do not comply with the criteria of CD but experiment intestinal symptoms and/or extra intestinal manifestations when consuming gluten. Recent studies have proposed that FODMAP (fermented oligo, di, monosacharides and polyols) as components of the wheat causing symptoms of NGCD, in addition to gluten.3 Its prevalence is estimated to be 10 times greater than CD. In Table 1 we expose the diagnostic criteria used to define NGCD.4 The gold standard for its diagnosis would be a double blind intervention controlled with placebo, because taking gluten out of the diet could lead to a placebo effect that may explain the improvement or remission of symptoms. In conclusion, we must take into account several considerations in the case presented by the authors. First, NGCD is a comorbid condition of FM/CFS, not the factor triggering it. Second, both FM and CFS are 2 chronic and complex diseases from the diagnostic and therapeutic standpoint, which require multidisciplinary management (adequate nutrition and dietary balance, symptom-based treatment, cognitive-conductual therapy and regulated gradual physical exercise) more than a simple GFD. Third, we believe that the case presented is a NGCD with extra intestinal affection (FM/CFS-like symptoms) more than FM/CFS per se.
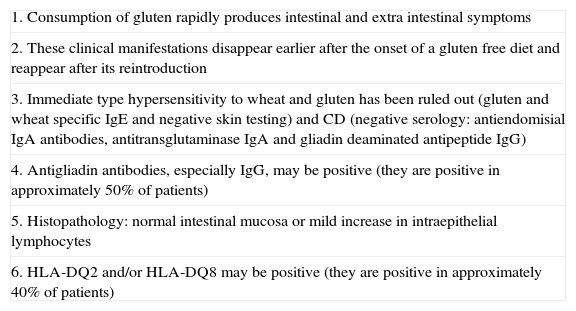
Diagnostic Criteria of Non-celiac Sensitivity to Gluten.
| 1. Consumption of gluten rapidly produces intestinal and extra intestinal symptoms |
| 2. These clinical manifestations disappear earlier after the onset of a gluten free diet and reappear after its reintroduction |
| 3. Immediate type hypersensitivity to wheat and gluten has been ruled out (gluten and wheat specific IgE and negative skin testing) and CD (negative serology: antiendomisial IgA antibodies, antitransglutaminase IgA and gliadin deaminated antipeptide IgG) |
| 4. Antigliadin antibodies, especially IgG, may be positive (they are positive in approximately 50% of patients) |
| 5. Histopathology: normal intestinal mucosa or mild increase in intraepithelial lymphocytes |
| 6. HLA-DQ2 and/or HLA-DQ8 may be positive (they are positive in approximately 40% of patients) |
CD, celiac disease.
Please cite this article as: Qanneta R, Fontova R, Castel A. Respuesta a: Fibromialgia y fatiga crónica causada por sensibilidad al gluten no celíaca. Reumatol Clin. 2015;11:185.


