








The burden of knee osteoarthritis (OA) in Latin America is unknown.
ObjectiveTo determine the demographic, clinical, and therapeutic characteristics of patients with OA in Argentina, Brazil, and Mexico.
Material and methodsThis is an observational, cross-sectional study of patients with symptomatic knee OA referred from first care medical centers to Rheumatology departments.
ResultsWe included 1210 patients (Argentina 398, Brazil 402, Mexico 410; mean age 61.8 [12] years; 80.8% females). Knee OA pain lasted for 69 months; the duration and severity of the last episode were 190 days and (SD 5.2 [3.3]; 74% had functional limitations, but very few patients lost their job because of knee OA. Around 71% had taken medications, but 63% relied on their own pocket to afford knee OA cost. Most demographic and clinical variables differed across countries, particularly the level of pain, disability, treatment, and access to care. The variable country of origin influenced the level of pain, disability, and NSAIDs use in logistic regression models; age, pain, treatment, and health care access influenced at least 2 of the models.
ConclusionsThe burden of knee OA in Latin American depends on demographic, clinical, and therapeutic variables. The role of such variables differs across countries. The level of certain variables is significantly influenced by country of origin and health care system.
La carga de la artrosis de rodilla (OA) en América Latina se desconoce.
ObjetivoDeterminar las características demográficas, clínicas y terapéuticas de los pacientes con OA en Argentina, Brasil y México.
Material y métodosSe trata de un estudio observacional, transversal, de pacientes con OA sintomática que son derivados de centros de atención primeria a los departamentos de reumatología.
ResultadosSe incluyeron 1.210 pacientes (Argentina 398, Brasil 402, México 410), con una media de edad de 61,8 (12) años; el 80,8% eran mujeres. El dolor de la OA de rodilla se prolongó durante 69 meses, la duración y la gravedad del último episodio fueron 190 días, y (DS 5,2 [3,3]; el 74% tenían limitaciones funcionales, pero muy pocos pacientes perdieron su empleo a causa de la OA de rodilla. El 71% había tomado medicamentos, pero el 63% lo pagó de su propio bolsillo. La mayoría de las variables demográficas y clínicas difieren entre los países, en particular el nivel de dolor, la discapacidad, el tratamiento y el acceso a la atención. La variable de país de origen influyó en el nivel de dolor, discapacidad y AINE a utilizar en los modelos de regresión logística; la edad, el dolor, el tratamiento y el acceso a la atención de salud influyó por lo menos a 2 de los modelos.
ConclusionesLa carga de la OA de rodilla en América Latina depende de las variables demográficas, clínicas y terapéuticas. El papel de estas variables difiere entre países. El nivel de ciertas variables se ve influido significativamente por el país de origen y el sistema de atención de la salud.
Osteoarthritis (OA) is the most common rheumatic disease in the general population and its prevalence increases with age.1,2 Genetic, mechanical, and several other factors have been implicated in its origin.3 OA symptoms such as joint pain, reduced mobility, crepitus, and swelling result from articular cartilage loss, subchondral bone proliferation, bone misalignment, and synovitis. The management of patients with OA includes a number of pharmacologic and non-pharmacological recommendations tailored in accordance to the joints involved.4–7 General physicians (GPs) see most patients with OA; referrals to specialized departments depend on surgical needs and patient preference.8
The knee is the largest joint most commonly involved in OA. The prevalence of knee OA ranges from 1.4% in urban Philippines15 to 19.3% in rural Iran16 whereas that of “painful knee OA” ranges from 6.5% to 28%.9–13 The age-standardized prevalence of knee OA is 1770 per 100000 males and 2693 per 100000 females.14 Along with hip OA, knee OA impairs physical functioning and decreases the quality of life of patients with OA.17–19 Mechanical factors, particularly those involved in the wear and tear processes in the joints, including body overweight and heavy-load work are major causes of the disease.20 There is an important association between knee pain and disability, which depends on the age of the patient, disease characteristics, and outcome measures.10–12,21
The prevalence and characteristics of OA in Latin America is partially known. Studies made according to World Health Organization/International League Associations for Rheumatology Community Oriented Program for the Control of Rheumatic Diseases (COPCORD) have shown a that the prevalence of OA in 2 Mexican studies is 2.3%22 and 10.5%,23 in Guatemala 2.8%,24 in Brazil 4.1%,25 in Peru 14.4%,26 and in Cuba 20.4%.27 Although these variations may reflect ethnical factors, it is also possible that methodological differences, demographic characteristics, and medical care accessibility might also influence those findings. Consequently, we developed an initiative for the study of knee OA in order to document its clinical features and consequences in patients living in Argentina, Brazil, and México. Specifically, we aimed to describe the level of symptoms and functional limitations in patients with clinical knee OA, the types of health care they access and the strategies followed in each country to deal with signs and symptoms of the disease.
Material and MethodsThis was an observational, cross-sectional study of patients with symptomatic knee OA carried out in Argentina, Brazil, and México. Institutional review boards at each country approved the protocol and informed consent of this study. The participants were informed about the nature of the study before signing an informed consent.
The population included in this study was a convenient sample of ambulatory patients with knee pain attributed to OA28 by trained General Physicians (GPs) in primary medical care units from where patients were referred to Rheumatology specialized departments in Argentina, Brazil, and Mexico in a 12-month period. Case definition referred to men and women >18 years old who complained of unilateral or bilateral weight bearing, non-traumatic, and non-inflammatory knee pain for >6 months and a current episode of continuous or sporadic knee pain of >1 month. Patients with a confirmed diagnosis of any active inflammatory rheumatic disease, including rheumatoid arthritis, spondyloarthritis, gout, calcium pyrophosphate dehydrate crystal deposition disease, connective tissue diseases, and infectious arthritis were not included in the study. Likewise, patients with congenital lower limb malformations, serious functional impairment, disability or chronic disease causing impaired functioning as consequence of foot, ankle, or hips involvement were not included in the study. The diagnosis of knee OA was established by GPs according to the American College of Rheumatology classification criteria.28 Patients’ assessment, including demographic data, clinical symptoms, physical function, health care utilization, and therapeutics was performed at the Rheumatology department.
We collected information on age, gender, occupation, height, weight, and body mass index (BMI). Ethnicity was operationally defined in accordance to parents and all 4 grandparents’ ethnicities as follows:29 (1) Whites: subjects with White European ancestors; (2) Mestizos: subjects with Amerindian and White European ancestors; (3) African Latin Americans: subjects who have at least one African ancestor irrespective of whether other ancestors were White or Amerindian; and (4) Pure Amerindians: subjects with all autochthonous ancestors.
Clinical variables included the duration of the disease and of the current episode of pain, its characteristics, and intensity in the last 6 months. We classified the localization of knee pain either as generalized (tenderness in all the knee) or localized (tenderness either in the internal, external, or patello-femoral aspects of the knee). We also looked for joint crepitus during movement and knee swelling. The assessment also included a characterization of diagnostic and therapeutic medical and non-medical interventions, type of health insurance coverage, and physical functioning using the Spanish version of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC).30 We also incorporated an item exploring the ability to perform activities of daily living and its relationship with keen pain as follows: (1) I do not have any problem to perform my normal daily activities, (2) I have some difficulties to perform some of my daily activities due to knee pain, (3) I have difficulties to perform most of my daily activities due to knee pain and (4) I am unable to perform most of my daily activities due to knee pain.
Statistical AnalysesGeneral and per country analyses were performed. These included descriptive and inferential analyses of demographic and clinical variables. Between-country comparisons were performed using analyses of variance (ANOVA) for normally distributed data and Kruskal–Wallis tests for non-normally distributed data. Categorical variables were compared using contingency tables. Three logistic regression analyses were conducted to determine the influence of gender, age, country of origin, ethnicity, BMI, duration of knee OA and of current pain episode, number of visits for medical consultation in the last year, drug prescription, and having medical insurance on pain (model 1), disability (model 2), and the use of non-steroidal anti-inflammatory drugs (NSAIDs) (model 3). The variable ability to perform daily living activities in relation with pain was dependent in the disability model 2 and independent in model 3. WOMAC total score was an independent variable of functioning in model 3. Statistical significance was set at a 0.05 alpha level. SPSS.17.0 was used to conduct all statistical analyses.
ResultsGeneral ResultsIn all, 1210 patients (mean age [±SD]: 61.8 [12.0] years) with knee OA were included in the study; 978 (80.8%) were females and 232 (19.2%) males (Table 1). Most patients were either Mestizos (50.9%) or Whites (36.9%). Nearly one third of the patients, mainly housewives worked at home; 47% were self-employed or had no employment at all and 10% were retired. Only 14.4% of the patients had a formal job.
General Characteristics Per Country and Total Population.*
| Argentina | Brazil | Mexico | P* | Total | |
| (n=398) | (n=402) | (n=410) | (n=1210) | ||
| Females | 340 (85.4) | 303 (75) | 335 (81.5) | 0.002 | 978 (80.8) |
| Males | 58 (14.6) | 99 (25) | 75 (18.5) | 0.002 | 232 (19.2) |
| Age, years, mean (SD) | 65 (10) | 57 (12) | 61 (11) | 0.000 | 61.8 (12) |
| BMI, mean (SD) | 29 (6.5) | 27 (5) | 27 (7) | 0.000 | 8 (6.4) |
| Ethnicity | (n=398) | (n=400) | (n=409) | 0.000 | (n=1207) |
| Mestizo | 142 (35.7) | 87 (21.8) | 386 (94.4) | 615 (51.0) | |
| White | 254 (63.8) | 182 (45.5) | 10 (2.4) | 446 (36.9) | |
| African-Latin-American | 0 (0) | 127 (31.7) | 3 (0.8) | 130 (10.8) | |
| Amerindian | 2 (0.5) | 4 (1) | 10 (2.4) | 16 (1.3) | |
| Work/job | (n=398) | (n=397) | (n=409) | 0.000 | (n=1204) |
| Works at home | 147 (36.9) | 109 (27.5) | 74 (18.1) | 330 (27.4) | |
| Unemployed | 61 (15.4) | 86 (21.7) | 176 (43.0) | 323 (26.8) | |
| Self employment | 72 (18.1) | 65 (16.4) | 108 (26.4) | 245 (20.3) | |
| Employee | 34 (8.5) | 109 (27.4) | 31 (7.6) | 174 (14.5) | |
| Retired | 80 (20.1) | 26 (6.5) | 12 (2.9) | 118 (9.8) | |
| Unable to work because of disease | 4 (1) | 2 (0.5) | 8 (2) | 14 (1.2) | |
n (%) unless stated otherwise.
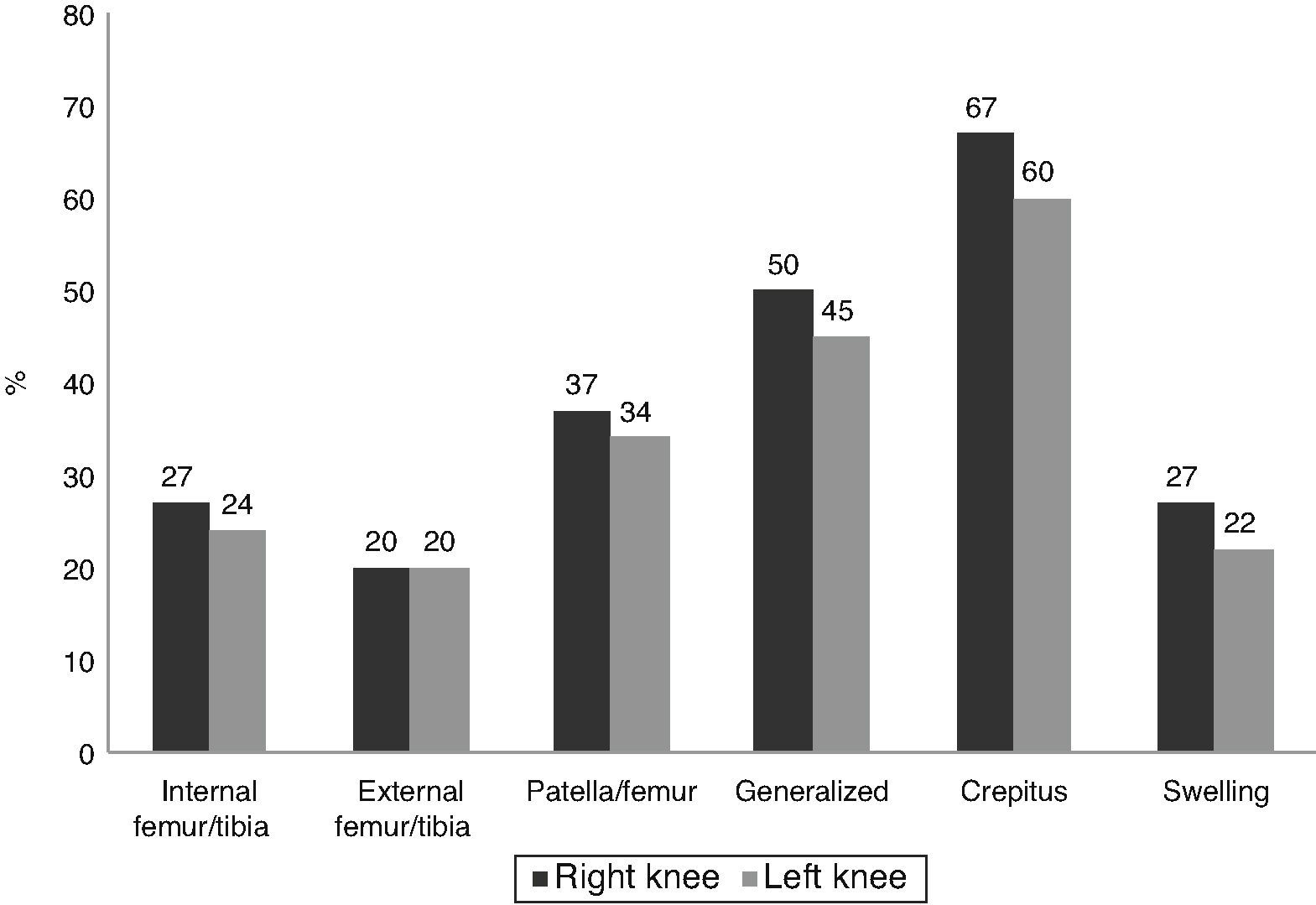
The mean total duration of knee pain was close to 6 years and the mean duration of the last episode was around 6 months (Table 2). Mean pain severity was 5.2 (3.3) on a VAS. Localization of pain did not differ between right and left knees, around one-half of the patients presented with generalized pain; localized pain occurred most frequently in the patella-femoral joint (Fig. 1). Nearly two-thirds of the patients had crepitus, and close to 25% presented joint swelling. Around 30% of patients had pain that worsened by climbing stairs; pain improved with rest in 52% of the patients. Although most patients experienced functional limitations, 26.6% reported no limitations at all (Table 3).
Characteristics of Pain and Its Consequences.*
| Argentina | Brazil | Mexico | P* | Total | |
| (n=398) | (n=402) | (n=410) | (n=1210) | ||
| Duration (months), mean (SD) | 63 (62) | 83 (83) | 60 (63) | 0.000 | 69 (70) |
| Duration, current episode (days), mean (SD) | 208 (409) | 141 (519) | 221 (542) | 0.04 | 190 (493) |
| Episodic | 308/396 (78) | 261/395 (66) | 295/401 (73) | 0.000 | 864/1192 (72) |
| Continuous | 88/396 (22) | 134/395 (34) | 106/401 (27) | 0.000 | 328/1192 (28) |
| Severity (VAS 0–10) | 6/2.2 | 5.1/2.6 | 4.6/4.5 | 0.000 | 5.2/3.3 |
| Pain worsening | (n=393) | (n=386) | (n=408) | 0.02 | (n=1187) |
| Climbing stairs | 140 (35.7) | 105 (27.2) | 97 (23.9) | 342 (28.8) | |
| Walking long distances | 45 (11.5) | 56 (14.5) | 51 (12.5) | 152 (12.8) | |
| Exercising | 43 (10.9) | 19 (4.9) | 74 (18.2) | 136 (11.4) | |
| Standing for long-time | 15 (3.8) | 34 (8.8) | 21 (5.1) | 70 (5.8) | |
| Bending | 14 (3.5) | 40 (10.3) | 12 (2.9) | 66 (5.5) | |
| Other | 136 (34.6) | 132 (34.3) | 153 (37.4) | 421 (35.7) | |
| Pain improvement | (n=394) | (n=386) | (n=406) | 0.07 | (n=1186) |
| Rest | 229 (58.2) | 206 (53.3) | 192 (47.2) | 627 (52.8) | |
| With medications | 71 (18) | 69 (17.8) | 116 (28.5) | 256 (21.5) | |
| No specific action | 19 (4.8) | 49 (12.6) | 9 (2.2) | 77 (6.4) | |
| Rest and medication | 23 (5.8) | 5 (1.2) | 29 (7.1) | 57 (4.8) | |
| Other | 52 (13.2) | 57 (15.1) | 60 (15) | 169 (14.5) | |
| Pain management | |||||
| Medications | 343 (86.2) | 222 (55.2) | 295 (72) | 0.000 | 860 (71.2) |
| Medications prescribed by a doctor | 316 (82.1) | 192 (47.7) | 255 (62.1) | 0.000 | 763 (63.2) |
| Took medication everyday in the last month | 137 (34.4) | 76 (19) | 115 (28) | 0.000 | 328 (27.2) |
| Days/month on medication, mean (SD) | 16.2 (11.5) | 11.9 (18.7) | 13.7 (13.4) | 0.000 | 13.9/15 |
n (%) unless stated otherwise.
Functional Status.
| Argentina | Brazil | Mexico | P* | Total | |
| Functioning | (n=397) | (n=390) | (n=410) | (n=1197) | |
| No limitations, n (%) | 102 (25.7) | 151 (38.7) | 68 (16.6) | 0.001 | 321 (26.8) |
| Some limitations, n (%) | 200 (50.4) | 157 (40.3) | 262 (63.9) | 0.001 | 619 (51.7) |
| Most activities limited, n (%) | 83 (20.9) | 68 (17.4) | 63 (15.4) | 0.001 | 214 (17.9) |
| Unable to do any activity, n (%) | 12 (3) | 14 (3.6) | 17 (4.1) | 0.001 | 43 (3.6) |
| WOMAC | (n=150) | (n=400) | (n=136) | 686 | |
| Total WOMAC index | 2.46 (1.66) | 1.17 (0.75) | 0.92 (0.69) | 0.000 | |
| Stiffness | 2.62 (2.06) | 1.1 (0.99) | 0.80 (0.81) | 0.000 | |
| Pain | 2.38 (1.81) | 1.2 (0.84) | 0.98 (0.74) | 0.000 | |
| Functioning | 2.35 (1.81) | 1.10 (0.80) | 0.99 (0.76) | 0.000 | |
Mean (standard deviation) unless stated otherwise.
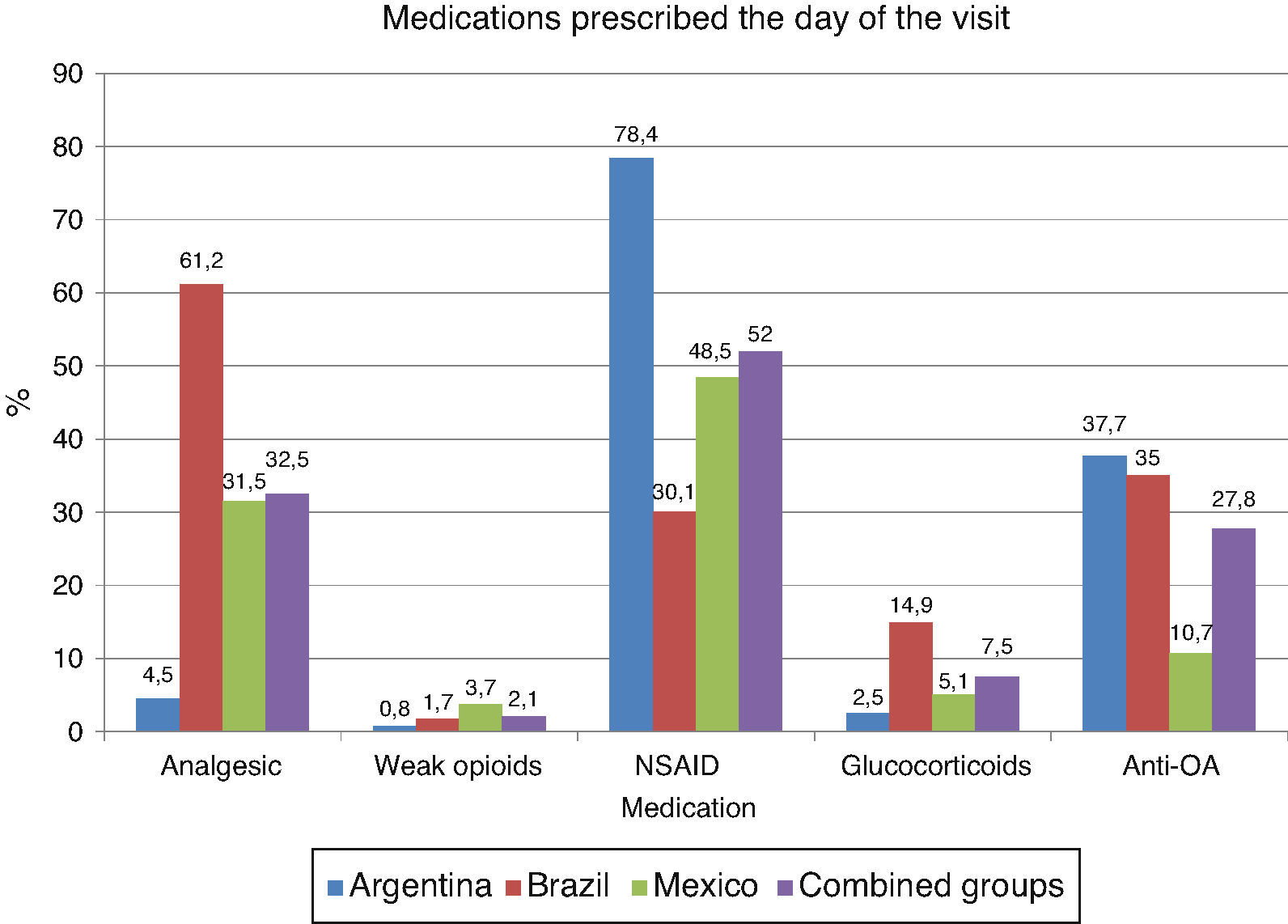
Despite most patients have a drug prescription for knee OA, few of them did actually take any medication within the last month (Table 2); 71% of the patients took medications for a mean of 13.9 months, but only 27% took them on a daily-basis in the previous month. Around 50% of patients were on NSAIDs, 32.5% on analgesics, and 27.8% on OA medications (Fig. 2). Less than 10% were on glucocorticoids or weak opioids for pain relief. NSAIDs were the most frequently prescribed drugs to control symptoms across the 3 countries. Compared with NSAIDs users (n=632), non-NSAIDs users (n=573) showed significantly higher levels of pain, WOMAC total and WOMAC subscale scores.
Despite all patients were referred by GPs, Rheumatologists have already seen 28% of them in the last 6 months (Table 4). In the same period, only 23% of the patients have being only seen by GPs. Other specialists, including orthopedic surgeons, treated nearly one-half of the participants. Interestingly, 56% of the patients came to ≤2 medical visits in the last 12 months.
Health Care Provision.*
| Argentina | Brazil | Mexico | P* | Total | |
| Medical care, last 6 months | (n=398) | (n=402) | (n=410) | .000 | (n=1210) |
| Primary care physician only | 85 (21.4) | 95 (23.6) | 154 (37.6) | 334 (27.6) | |
| Rheumatologist only | 163 (41.0) | 48 (11.9) | 66 (16.1) | 277 (22.9) | |
| Orthopedic surgeon only | 0 (0) | 17 (4.2) | 9 (2.2) | 26 (2.1) | |
| Others | 150 (37.6) | 242 (60.3) | 181 (44.1) | 573 (47.4) | |
| Medical visits, last 12 months | (n=398) | (n=398) | (n=409) | .36 | (n=1205) |
| One | 74 (18.6) | 97 (24.4) | 102 (24.9) | 273 (22.7) | |
| Two or three | 165 (41.5) | 110 (27.6) | 139 (34.0) | 414 (34.3) | |
| Four or more | 159 (39.9) | 191 (48.0) | 168 (41.1) | 518 (43.0) | |
| Health insurance | (n=397) | (n=396) | (n=405) | .000 | (n=1198) |
| None | 113 (28.5) | 267 (67.4) | 384 (94.8) | 764 (63.8) | |
| Partial | 229 (57.7) | 34 (8.6) | 12 (3.0) | 275 (23.0) | |
| Complete coverage | 55 (13.8) | 95 (24.0) | 9 (2.2) | 159 (13.2) | |
Nearly two-thirds of the patients had no access to any institutional or socialized medical care system and had to rely on their own pocket to cover the cost of their disease; 23% of the patients had partial coverage (medications not included) and only 13% had a full medical care coverage (medications included).
Results Across PopulationsComparisons between countries disclosed significant differences in most demographic and clinical variables. There were more males among Brazilians and older age of OA onset in Argentinians (Table 1). The proportion of employees was much higher (27.1%) in Brazil, whereas the highest proportion of self-employed and unemployed patients was found in Mexico. Regarding ethnicity, there were more Whites in Argentina, more African Latin Americans in Brazil, and more Mestizos in México. Although the total duration of pain was longer in Brazil, the duration of the last episode of pain was shorter in Brazilians than in Argentinians and Mexicans (Table 2). The intensity of pain and the proportion of patients with pain worsening by climbing stairs were higher among Argentinians. The proportion of Mexican patients with physical limitations was higher than those among Brazilians and Argentinians (Table 3). Argentinians had the highest proportion of patients taking prescribed and non-prescribed medications as well as the longest time on treatment (Table 2). The proportion of NSAIDs consumption was higher in Argentina, but the consumption of analgesics and glucocorticoids was much lower than in Brazil and Mexico. The consumption of anti-OA medications was much lower among Mexicans.
There were significant differences in-between the 3 countries in regard to health care provision (Table 4). More patients with knee OA were seen by Rheumatologists and more patients had partial or full health care coverage in Argentina. In contrast, more than 90% of the patients in Mexico relied on their own pocket to afford the cost of health care.
Logistic Regression Models of Pain, Disability, and NSAIDs UsePain model: the ability of this model to distinguish between patients with pain above or below 5.2 on VAS was statistically significant (P=.000). The variables that contributed to this model were country of origin, having a drug prescription and the number of medical visits in the last year (Table 5). Disability model: with this model we were able to distinguish patients with and without disability (P=.000). The independent variables that significantly influenced this model were country of origin, drug prescription, number of medical visits in the previous year, age, BMI, ethnicity, pain level, and having medical insurance (Table 5). NSAIDs usage model: The ability of this model was statistically significant (P=.000) in distinguishing patients with and without NSAIDs prescriptions. Only country of origin, age, and pain level made a significant contribution to the model (Table 5).
Summary of the Results of Regression Analyses, With Regression Coefficients for the Predictor Variables for Pain ≥ 5.2, Disability, and Non-steroidal Antinflammatory Drugs Use.
| b | SE | P | OR | 95% CI | ||
| Pain ≥5.2 on a visual analog scale | ||||||
| Country | .000 | |||||
| Argentina | 1.244 | .208 | .000 | 3.469 | 2.309 | 5.211 |
| Brazil | .978 | .210 | .000 | 2.660 | 1.762 | 4.015 |
| Medical visits last year | −.179 | .085 | .035 | .836 | .708 | .988 |
| Having treatment | 1.034 | .157 | .000 | 2.812 | 2.068 | 3.823 |
| Disability | ||||||
| Country | .000 | |||||
| Argentina | −1.459 | .276 | .000 | .232 | .135 | .399 |
| Brazil | −1.492 | .259 | .000 | .225 | .135 | .374 |
| Age | .027 | .007 | .000 | 1.028 | 1.013 | 1.042 |
| Body mass index | .028 | .012 | .025 | 1.028 | 1.003 | 1.053 |
| Ethnic group | .002 | |||||
| Amerindian | −1.548 | .689 | .025 | .213 | .055 | .820 |
| Caucasian | −1.060 | .291 | .000 | .347 | .196 | .613 |
| Mestizo | −.754 | .315 | .017 | .471 | .254 | .872 |
| Medical visits last year | .572 | .104 | .000 | 1.771 | 1.445 | 2.171 |
| Having treatment | .783 | .175 | .000 | 2.187 | 1.552 | 3.083 |
| Medical insurance | .035 | |||||
| None | −.590 | .246 | .017 | .554 | .342 | .898 |
| Pain VAS | .257 | .033 | .000 | 1.293 | 1.213 | 1.379 |
| Taking non steroidal antinflammatory drugs | ||||||
| Country | .000 | |||||
| Argentina | 1.088 | .233 | .000 | 2.970 | 1.880 | 4.692 |
| Brazil | −1.216 | .227 | .000 | .297 | .190 | .463 |
| Age | −.019 | .006 | .003 | .981 | .969 | .994 |
| Duration | .002 | .001 | .037 | 1.002 | 1.000 | 1.004 |
| Pain | .181 | .028 | .000 | 1.198 | 1.134 | 1.265 |
SE=standard error; OR=odds ratio; CI=confidence interval.
We have assessed the characteristics of knee pain related to OA and its impact on 1210 patients referred from primary health clinics to Rheumatology departments in Argentina, Brazil, and México. Rather than finding a common pattern, our study showed important differences in the frequency of most demographic and clinical variables. Some of such differences have already been described Latin American studies of patients with systemic lupus erythematosus,29 spondyloarthritis,31 and early rheumatoid arthritis32 and have been explained of the basis of ethnical, environmental, and demographic factors. In addition, the role of educational, socioeconomic factors, and health care system should also be considered.33
Nevertheless, general assumptions in this study include the onset of knee OA pain before the age of 65 years and more women than men affected by the disease. Despite a small proportion of our patients had a formal job, very few had lost it because of the disease. Only 4% of the patients were unable to do any physical activity and 25% had low WOMAC scores and no physical limitations at all. These findings suggest that the severity of knee OA in our study was actually mild to moderate and that its pattern is certainly similar to that of patients attending primary care units in which OA referrals to specialized departments depends on the need for joint replacement, physical therapy and rehabilitation, comorbidities management, and demographic factors.8,34–40 Despite all patients in our study were under the care of GPs, most of them were already seen by rheumatologists and orthopedic surgeons.
The overall and last episode of pain lasted for more than 5 years and around 6 months, respectively and their intensity was 5.2 on a VAS. These findings seem to agree with studies suggesting that the longest the duration of knee OA complaints, the higher the intensity of pain.40,41 In the regression model, having knee pain >5.2 was associated with being treated in Argentina or Brazil, the number of medical visits in the last year, and having a drug prescription for knee pain.
Nearly 3 quarters of the patients had taken medications throughout the course of the disease, but very few took them on a daily basis; 52% had taken NSAIDs, 32.5% non-narcotic analgesics, and 27.8% anti-OA medications. The consumption of analgesic and NSAIDs relied on the severity of symptoms than on a regular basis schedule. Analgesic and NSAIDs prescription in patients with knee OA has been linked to disease perception,8 age, gender, medical and social contexts,42 health care utilization and health professional contact,37,39 performance of heavy load tasks,43 and need of surgical treatment.44 In our study, the level of pain, age, and country of origin were associated with NSAIDs’ prescription in the regression analysis. Finally, 30% of the studied population received OA modifying drugs, but differences between countries were also found. Overall, the therapeutic approach for knee OA in this study seems consistent with current recommendations for the management of the disease.4–7
Several studies have shown that age, gender, BMI, number of co-morbidities, type of job, access to medical care, and disease duration in patients with knee OA are associated with reduced HRQoL, poor functioning, job loss, and increased burden of disease.17–19,45–55 Except for those cases requiring surgery, the radiographic features in knee OA do not correlate with clinical findings and do not determine HRQoL or physical functioning.45,49,51,52
Comparisons between countries yielded some interesting differences in demographic characteristics, health care utilization, and some clinical and therapeutic features. This should not be unexpected since previous studies have linked the characteristics of knee OA to ethnicity, living conditions, and access to care.14,20,35,37–40,55–60 As consequence the fragmentation of the health system in Latin America, only a variable percentage of the population is either fully or partially covered by the state. For those who are partially covered and those who are not covered by any of such systems, the cost of disease is paid with their own money, either through direct payments or the acquisition of a private medical insurance. Health care access is limited and the burden of disease for the patient and householders is huge.61 Enabling variables, such as pain and reduced function and not the need of care have a direct effect on the utilization of health service, specifically the availability of health coverage, the existence of a regular source of care, and the out-of-the pocket money. This finding might indicate that patients with chronic diseases such as knee OA do not only learn to live with their disease, recognizing their symptoms, but also know how to deal with the health-care system.
We were interested in the role of some of such as well as other independent variables in pain level, disability, and use of NSAIDs. The contribution of country origin was significant in all 3 logistic regression models. Patients from Argentina were over 3 times more likely to report pain ≥5.2, but were 2.97 times more likely to be on NSAIDs than Mexicans. Compared with Mexicans, Brazilians were 0.29 and 0.22 times less likely to be on NSAIDs or present disability than Mexicans. Argentinians were 0.23 times less likely to present disability than Mexican patients. The significance of the variable country of origin as predictor of pain level, disability, and NSAIDs usage might support the role of each country health-care systems and less likely ethnicity in the burden of knee OA.
For every additional medical visit, patients were 0.83 times less likely to report pain ≥5.2, but 1.7 times more likely to present disability. Each incremental unit in VAS pain was associated with 1.29 and 1.19 more chances of being on NSAIDs and having disability. Patients who had a drug prescription were 2.8 times more likely to present pain equal or above to 5.2 on a VAS and 2.18 times more likely to present disability. For each year increment on age there is a 0.98 times less chance to receive NSAIDs in this population.
There were some potential limitations to our study. Regarding the representativeness of the populations included in our study, our approach was the identification of knee OA at primary health care clinics. In this regard, we followed the usual steps took by the patients with knee OA in the 3 countries. Following a standard protocol, GPs referred consecutive knee OA patients to the rheumatologist for detailed characterization of demographic and clinical variables. Differences between countries in regard to demographic and access to care seemed to reflect the characteristics of the population and health care in each of the 3 countries.
In conclusion, the burden of knee OA in Latin American countries seems to be related with demographic factors, including the characteristics of the health system. Knee OA in primary health clinics seems to be a mild form of disease with mild impact on functioning. At this stage, knee OA could be the target of disease modifying agents as treatment. We think that the assessment of disease, particularly knee OA should include the individual analysis of each Latin American country. By following that approach, health care planning, from detection of disease to its treatment would be more appropriate to the needs of each country.
Source of FundingSupported by an unrestrictive fund from Expanscience Laboratories.
Conflict of InterestHafid Halhol is employed by Laboratories Expanscience. The other authors declare no conflict of interest.
Ethical ResponsibilitiesProtection of Human and Animal SubjectsThe authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Confidentiality of DataThe authors declare that they have followed the protocols of their work center on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to Privacy and Informed ConsentThe authors have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.


