

Osteoarthritis causes severe pain and disability in joints, one of the most prevalent involved joints is the knee joint. There are several therapeutics ways to control pain and disability, but almost none of them are definite treatment. In this article, we tried to reveal the effect of weight loss on improving symptoms of knee osteoarthritis as an effective and permanent therapeutic approach.
MethodsWe chose 62 patients with grade 1–2 (mild to moderate) knee osteoarthritis and divided them equally into case and control groups. Patients should not had used NSAIDs at least for 6 months before study initiation. Symptoms severity was measured by WOMAC and VAS questionnaires before and after 3 months follow up. Weight and BMI were recorded too. Case group was suggested to have weight loss diet of less fat and carbohydrates and control group did not have any limitation.
ResultsComparison of variables’ average of case and control groups was not logistically meaningful at the initiation and after the end of the study. But there was a meaningful correlation between variables’ changes and lifestyle change in both groups, especially in WOMAC and VAS scores. All variables in case group had statistically meaningful differences between their amounts at the beginning and after the end of the study, on the contrary of the control group.
ConclusionIn the comparison of our study with similar studies in the world. We deduced that weight loss can improve symptoms of knee osteoarthritis even in short time weight loss diet (3 months).
Trial registration numberZUMS.REC.1394.94.
La osteoartritis causa dolor e incapacidad articulares severos. Una de las articulaciones con mayor prevalencia es la rodilla. Existen diversos enfoques terapéuticos para controlar el dolor y la incapacidad, pero ninguno de ellos constituye un tratamiento definitivo. En el presente artículo, tratamos de demostrar el efecto de la pérdida de peso sobre la mejora de la osteoartritis de rodilla, como enfoque terapéutico efectivo y permanente.
MétodosElegimos a 62 pacientes con osteoartritis de rodilla de grado 1-2 (de leve a moderado), dividiéndolos equitativamente entre el grupo de casos y el grupo control. Los pacientes no debían haber utilizado AINE al menos durante los 6 meses previos al inicio del estudio. La gravedad de los síntomas se midió mediante los cuestionarios WOMAC y VAS al inicio del estudio, y durante el seguimiento a los 3 meses. También se registraron el peso y el IMC. Se recomendó al grupo de casos que siguieran una dieta baja en grasas y carbohidratos para perder peso, y al grupo de control no se le indicó limitación alguna.
ResultadosLa comparación de las medias de las variables de los grupos de casos y controles no fue logísticamente significativa al inicio y al final del estudio, pero sí se produjo una correlación significativa entre los cambios de las variables y el cambio de estilo de vida en ambos grupos, especialmente en las puntuaciones WOMAC y VAS. Todas las variables del grupo de casos reflejaron diferencias estadísticamente significativas entre los valores al inicio y al final del estudio, al contrario que en el grupo control.
ConclusiónEn la comparación de nuestro estudio con estudios similares a nivel mundial dedujimos que la pérdida de peso puede mejorar los síntomas de la osteoartritis de rodilla, incluso en dietas para pérdida de peso de corta duración (3 meses).
N.° de registro del ensayoZUMS.REC.1394.94.
Osteoarthritis (OA) is one of the causes of pain and disability in the most of the rheumatology patients. It causes progressive degeneration of joint's cartilage and decreases joint space.1 It is considered to involve all parts of synovial joint but the most important hallmark is cartilage damage.2 Appropriate approach for diagnosing OA is using of clinical signs and symptoms and radiographic pictures.3
Knee osteoarthritis is the most prevalent chronic joint disease which leads to arthralgia and changes in the shape of joint and finally causes patient disability. This disease is classically defined as focal joint cartilage lesion which is accompanied by the subchondral bone hypertrophic reactions.4 Risk factors of knee OA are female gender, genetically predisposition, overweight and history of knee injury.5 13.7 million persons in United States of America have symptomatic knee osteoarthritis.6 Symptomatic knee osteoarthritis prevalence in men and women with age of more than 80 years old is 16% and 5.4%, respectively, and generally, 11% of persons older than 64 years have it.4
Due to the high prevalence and progressive essence of the diseases which leads to the disability of patient and rising the therapeutic expenditures, there are lots of efforts for treating this disease. Most of the drugs which are used in OA treatment are just symptoms reliever. Knee OA treatments are dividing into two categories: drugs and nondrug methods. Nondrug methods are the teaching to the patients for using their joints better, how to consider their joint statement in their daily life and work, muscle strengthening exercises, aerobic exercises and body weight loss, thermotherapy and acupuncture. Drug treatments are oral and local injection of NSAIDs, acetaminophen, intra-articular injections of corticosteroids and hyaluronic products and supplements such as glucosamine and chondroitin sulfate.7 There are some other newer treatments which their effectiveness have been shown such as autologous mesenchymal stromal cells (MSC), adipose-derived stem cell treatment, leukocyte-poor platelet-rich plasma (LP-PRP), and others.8–10
The aim of this study is determining weight loss efficacy on the improvement of knee OA patients’ clinical status.
Material and methodsThis study was registered at the ethic committee of the Zanjan University of Medical Science and approval number is ZUMS.REC.1394.94. We have obtained written consent from all patients.
Study type is randomized controlled clinical trial (RCT) and was carried out on 62 patients which were divided equally into case and control groups (31 vs. 31). This study started in January 2015 and ended in August 2015 at Vali-e-asr hospital, Zanjan, Iran. Knee osteoarthritis was approved according to ACR ranking criteria.
InclusionThe severity of joint involvement was in grades 1–2 (mild and moderate) according to Kellgren & Lawrence system. Osteoarthritis considered on the base of existence of mechanical pain in the knee, joint crepitation sensing through physical examination and radiographic signs. The participated patients did not have any disease other than knee osteoarthritis.
ExclusionPatients with below characteristics were excluded, these characteristics were knee and hip joint prosthesis, consumption of glucosamine and chondroitin sulfate drugs through last 6 months, overuse of sedative drugs, 3–4 OA grades and rheumatic diseases history. The existence of aforementioned characteristics was assessed by patients’ records, asking from patients, physical examination, and radiological workups. Patient with comorbidities were detected by questionnaire, laboratorial tests and physical examinations then they were excluded of the study.
InterventionPatients were divided into two groups according to their BMI, age, sex and their osteoarthritis intensity; then they placed randomly four blocks in intended groups by the Block Randomization method. The first group was suggested using less starch, rice, spaghetti, fatty foods, solid and liquid oil. We did not suggest anything to the second group. We emphasized patients to not to use edative drugs and if they absolutely had to, they were asked to write the name and dosage in provided sheets. For ensuring of patients collaboration with study and correct implementation of suggestions and not taking sedative medications, we made calls with patients every month.
OutcomesThe primary outcome was weight loss and the secondary was decreased pain which were measured as follows. At the beginning of the study, patients’ weight was measured with calibrated balance and height was measured in centimeters and BMI was calculated. Symptoms intensity assessed by WOMAC (Western Ontario and McMaster universities) and VAS (Visual Analog Scale) questionnaire and were followed up for 3 months. After the end of the study, body weight was measured with the same scale and WOMAC and VAS questionnaires were filled again.
Statistical methodsInformation was extracted by questionnaire and analyzed by SPSS version 20 software. Quantitative data with normal distribution were analyzed by independent T-test and quantitative data without normal distribution were analyzed by Mann–Whitney test. Each patient was compared with him/herself and other groups and analyzed for effect of weight losing on their knee OA symptoms relieve. We anticipated that each patient in the group with restricted nutrition would lose 1kg each month.
Results62 patients with knee OA participated in the study, which was divided into case and control groups (31 vs. 31). 3 (9.7%) patients were male and 28 (90.3%) were female in each group. 15 (48.4%) and 13 (41.7%) of patients had stage 1 disease in control and case groups, respectively. Others had stage 2 disease in each groups. 1 (3.2%) and 5 (16.1%) of patients had used sedative drugs before study in control and case groups, respectively. Others had not used sedative drugs in each group. Mean age of case group patients was 48±8.1 and of control group was 44.5±8.9 years old.
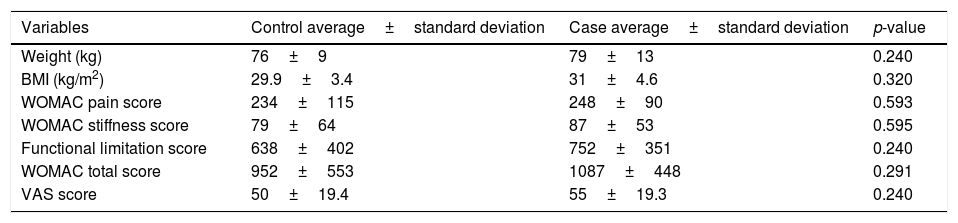
All studied variables including weight, BMI, WOMAC pain score, WOMAC stiffness score, functional limitation score, VAS score, and WOMAC total score at the beginning of the study had not any significant differences between case and control groups (Table 1).
Comparison of variables of case and control groups before beginning the intervention.
| Variables | Control average±standard deviation | Case average±standard deviation | p-value |
|---|---|---|---|
| Weight (kg) | 76±9 | 79±13 | 0.240 |
| BMI (kg/m2) | 29.9±3.4 | 31±4.6 | 0.320 |
| WOMAC pain score | 234±115 | 248±90 | 0.593 |
| WOMAC stiffness score | 79±64 | 87±53 | 0.595 |
| Functional limitation score | 638±402 | 752±351 | 0.240 |
| WOMAC total score | 952±553 | 1087±448 | 0.291 |
| VAS score | 50±19.4 | 55±19.3 | 0.240 |
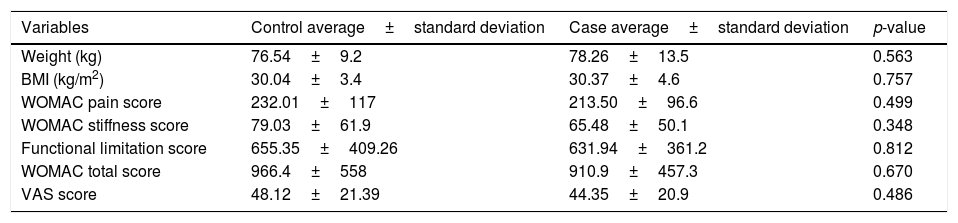
As shown in Table 3, there are not any meaningful differences between case and control groups’ averages of weight, BMI, WOMAC pain score, WOMAC stiffness score, functional limitation score, VAS score, and WOMAC total score, after applying the intervention (Table 2).
Comparison of final variables amount of control and case groups after ending the intervention.
| Variables | Control average±standard deviation | Case average±standard deviation | p-value |
|---|---|---|---|
| Weight (kg) | 76.54±9.2 | 78.26±13.5 | 0.563 |
| BMI (kg/m2) | 30.04±3.4 | 30.37±4.6 | 0.757 |
| WOMAC pain score | 232.01±117 | 213.50±96.6 | 0.499 |
| WOMAC stiffness score | 79.03±61.9 | 65.48±50.1 | 0.348 |
| Functional limitation score | 655.35±409.26 | 631.94±361.2 | 0.812 |
| WOMAC total score | 966.4±558 | 910.9±457.3 | 0.670 |
| VAS score | 48.12±21.39 | 44.35±20.9 | 0.486 |
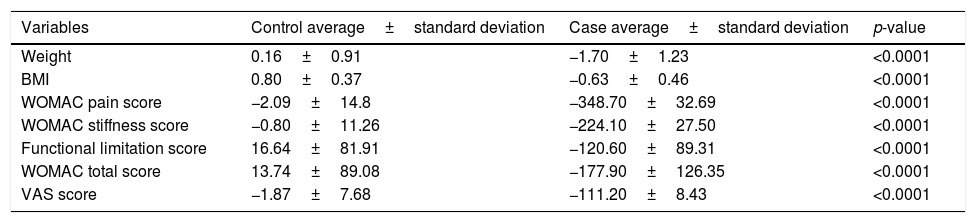
According to Table 3, changes of weight, BMI, pain score, stiffness score, functional limitation score, VAS score and total WOMAC score in control and case groups have statistically meaningful relations (Table 3).
Comparison of variables’ changes of control and case groups after ending the study.
| Variables | Control average±standard deviation | Case average±standard deviation | p-value |
|---|---|---|---|
| Weight | 0.16±0.91 | −1.70±1.23 | <0.0001 |
| BMI | 0.80±0.37 | −0.63±0.46 | <0.0001 |
| WOMAC pain score | −2.09±14.8 | −348.70±32.69 | <0.0001 |
| WOMAC stiffness score | −0.80±11.26 | −224.10±27.50 | <0.0001 |
| Functional limitation score | 16.64±81.91 | −120.60±89.31 | <0.0001 |
| WOMAC total score | 13.74±89.08 | −177.90±126.35 | <0.0001 |
| VAS score | −1.87±7.68 | −111.20±8.43 | <0.0001 |
Weight and BMI averages at initiation (79.9±13.9) and end of the study (78.2±13.5) in case group has meaningful statistical differences (p<0.0001). BMI averages at initiation (31±4.6) and end of the study (30.37±4.6) in case group has meaningful statistical differences (p<0.0001). But these differences in the control group are not statistically meaningful.
All variables after and before the intervention, in case group have statistically meaningful differences. But differences in control groups are not meaningful.
Discussion62 patients with knee OA participated in the study and were divided into case and control groups (31 vs. 31) and were analyzed. Average weight loss of 3 months in case group was 1.7kg and it was not equal to anticipated amount and, also, some patients in control group had autonomous weight loss. Thus, at the end of the study, the average of pain, stiffness, functional limitation, VAS and total WOMAC scores in both groups had not meaningful differences, but averages of their changes between two groups were meaningful (p<0.0001). Averages of studied variables’ scores in case group at initiation and end of the study were statistically meaningful (p<0.0001) which shows the effectiveness of weight loss in the improvement of clinical symptoms of patients. In a study by Robin et al. in 2007 on 454 patients with knee OA, they showed that with decreasing more than 6.1% of body weight in obese patients with knee OA, they can highly relieve their pain and improve their function and disability (p<0.0001) which is an approval for weight loss effectiveness on the improvement of patients’ symptoms as ours.11
In a study by Gudbergsen et al. in 2011 on 192 patients with knee OA, they divided patients into two groups and suggested 16 weeks weight losing diet to case group. They concluded that decreasing body weight can relieve symptoms at any stage of the disease.12 This study had the larger sample size and longer duration in comparison to ours, but our study showed positive effects of weight losing despite its smaller study groups population and shorter follow-up time.
In a study by Aaboe et al. in 2011 on 157 obese patients with knee OA, they concluded that decreasing in body weight by 13.7kg in 16 months can significantly relieve exerted pressure on the knee joint and improves functional ability of patients with knee OA (p<0.0001).13 This study had larger sample size and longer duration in comparison to ours, but our study showed positive effects of weight losing on WOMAC questionnaire components such as stiffness, functional limitation and pain, despite its smaller studied population and shorter follow-up. It showed symptoms improvement in patients with knee OA with weight loss as our study shows.
In a study by Coriolano et al. in 2013 on 34 obese female patients with knee OA, they suggested weight loss diet to patients and followed them up for 6 months and gathered needed data with WOMAC questionnaire. They showed that at least 16.5% loss of body weight could be enough for improving symptoms especially pain, and, also could postpone surgery operations in patients that were intended to have that.14 Our study shows the same results beside that we had a larger population and shorter intervention interval.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
ContributionsDr. Zahra Abbaspour Rad: Conception and design, and analysis and interpretation of the data;
Dr. Behnam Sajedi: Drafting of the article;
Dr. Amir Hossein Heydari: Critical revision of the article for important intellectual content and Drafting of the article;
Dr. Samira Akbarieh: Collection and assembly of data;
Dr. Behzad Jafari: Collection and assembly of data;
Dr. Alireza Sadeghi: Analysis and interpretation of the data and final approval of the article.
Conflict of interestNone of the mentioned authors have financial interest in this paper and there is not any commercial or financial relevance between any of the authors with third person or institution. Zanjan University of Medical Science has paid a portion of costs as grant for thesis costs. There is no need to report article submission progression to aforementioned institution.
We appreciate all patients their family and Vali-e asr hospital personnel for helping us to do this study.
The following are the supplementary data to this article:


