


The beneficial effects of exercise in the treatment of Osteoarthritis (OA) of the knee have been verified in several studies. Kinesiotaping (KT) has been popularized due to its reducing local pressure and increasing circulation, resulting in decreased pain.
ObjectiveDetermine the clinical effectiveness of strengthening therapy with KT in women with knee OA for pain reduction.
MethodsThirty two women with knee OA, aged 50–70 years, with overweight or obesity grade I, who were randomized into two groups: one with exercise and KT, and the other, with exercise and placebo technique. Both groups performed stretching and quadriceps strengthening exercise with the elastic band 3 days weekly for 6 weeks. Measurement of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain subscale was taken as primary outcome. Stiffness and functionality of the same index and the Visual Analog Scale (VAS) for pain intensity were measured.
ResultsAt the end of the study, there were no significant differences between the groups. Both groups had a difference of 2.7 points with respect to the baseline measurement, change percentage of 32.2% and 31.1% for placebo and experimental respectively (p=0.2).
ConclusionsKT plus quadriceps strengthening exercise does not offer advantages for improvement of pain compared with quadriceps strengthening exercise alone in knee OA.
Los efectos benéficos del ejercicio en el tratamiento de la osteoartritis (OA) de rodilla han sido verificados en varios estudios. El vendaje kinesiológico o kinesiotaping (KT) se ha popularizado debido a la reducción de la presión local y el aumento de la circulación, lo que resulta en disminución del dolor.
ObjetivoDeterminar la efectividad clínica de la terapia de fortalecimiento en conjunto con el uso de KT en mujeres con OA de rodilla para la reducción del dolor.
MétodosParticiparon 32 mujeres con OA de rodilla, con edades comprendidas entre 50 y 70 años, sobrepeso u obesidad grado I, que fueron asignadas al azar en 2 grupos: uno con ejercicio y KT y otro con ejercicio y vendaje placebo. Ambos grupos realizaron ejercicios de estiramiento y fortalecimiento de los cuádriceps con banda elástica 3 días semanales durante 6 semanas. El desenlace primario fue medido con la subescala del dolor del Western Ontario y McMaster Universities Osteoarthritis Index (WOMAC). Se midieron la rigidez y la funcionalidad del mismo índice y la escala analógica visual (VAS) para la intensidad del dolor.
ResultadosAl final del estudio, no hubo diferencias significativas entre los grupos. Ambos grupos tuvieron una diferencia de 2,7 puntos respecto a la medición basal, porcentaje de cambio del 32,2 y 31,1% para placebo y experimental, respectivamente (p=0,2).
ConclusionesEl KT en conjunto con el ejercicio de fortalecimiento no ofrece ventajas para mejorar el dolor en comparación solo con el ejercicio de fortalecimiento en la OA de rodilla.
Osteoarthritis (OA) is a common joint disease. It is an important source of pain and knee failure in the old population1 and is characterized by the loss of biochemical integrity and function of articular cartilage. The knee is the main site of OA.2,3 The incidence of knee OA standardized by age is 240 per 100,000 person-years and women have an increased risk of OA, particularly for knee and hand OA.4 At the non-pharmacological level, actions such as exercise are considered more appropriate.5,6 Among the latter, exercise plays an important role in reducing pain; thus, its inclusion has become essential in the treatment7–9 and the execution of exercise with elastic band has proved to be a viable and effective option.9–11 On the other hand, Kinesio Taping (KT) is currently a technique that has generated a new trend in the treatment of pain, strength, functionality and other outcomes related to skeletal muscle and joint injuries,12,13 The popularity of KT demands special consideration in terms of its popularity because, in the last decade, there has arisen a great amount of distributors offering KT related seminars, courses, products and accessories.14,15 Previous studies have been conducted for the outcome of pain in various clinical conditions (knee, shoulder, neck, spine, plantar fascia) with different methodologies and results, giving different qualities of evidence also, so the application of KT continues to have little value among clinicians.16 There have been some preceding studies of KT effects over the OA,17–23 where the exercise is not present or does not play an important role due to the short duration of the interventions. So, we consider important to emphasize the incorporation of the exercise when carrying out an investigation of these characteristics.
The aim of this study was to determine the effectiveness of KT along with exercise therapy in women with OA.
Materials and methodsA single center randomized clinical trial, single blind, 6 weeks duration was conducted. Inclusion criteria: women aged between 50 and 70 years, with BMI between 25 and 34.9, and diagnosed with bilateral knee OA according to European League Against Rheumatism (EULAR) criteria, classified as grade 2 or 3 by the radiographic scale of Kellgren and Lawrence.24 It is important to note that although OA was bilateral, only the most affected knee was evaluated. Exclusion criteria: knee joint replacement: pain associated with other knee injuries; strengthening therapy at the time of intervention; <90° knee flexion; known sensitivity to tape materials, or contraindication for exercise.
Assignment and randomizationA member of the research team generated a randomized list of 32 patients assigned to two groups. The randomization method used was by blocks. Free license software, recommended by Suresh25 and available at www.randomization.com was used. In this study, the number of patients per block was 4, with a total of 8 blocks, thus considering the 30 patients calculated for the sample size and two more that were added to balance the groups. 32 opaque envelopes containing a card with two possible legends were listed: A (experimental) or B (control). The envelopes were previously delivered to another member of the team (blinded), located in another hospital, who by telephone transmitted the assignment to a sports doctor (not blinded) who gave the participants instructions regarding the intervention that would be given to them (taping technique and exercise).
WOMAC scaleTo determine the change in the degree of knee pain, the WOMAC scale was applied. This scale consists of three dimensions: pain, stiffness and functionality. It is graded with a Likert scale of 0–4 and a higher score denotes a worst situation (96 points – 20 for pain, 8 for stiffness and 68 for functionality). Several studies have been published about its reliability.26
InterventionThe exercise intervention was based on the quadriceps strengthening program published by Chang et al.9 We developed a program in which the patients performed a dynamic-type strengthening exercise (6–8 per Omni Perceived Exertion Scale-Resistance Exercise Scale [OMNI-RES]) in their home, with a volume of 3 sets of 15 unilateral repetitions, with extension and flexion movement for both knees (2-s duration per movement), with a frequency of twice a day. For calculation of 1-Repetition Maximum (1RM), a red, green, or blue band test (Theraband®) was performed, requesting that the patient perform at least 10 repetitions of extension. The band was tied to a belt worn by the participant, which that would aid in stabilizing the exercise. The participant leaned against a wall, sitting on the floor with both knees in extension. They were asked to flex and adjust the elastic band to generate tension against the extension of the knee. The band was adjusted to the level of effort requested according to the OMNI-RES scale.13 With this elastic band, the participants performed, in their homes, 3 sets of 15 repetitions of extension and 3 sets of 15 repetitions of knee flexion unilaterally. Rest intervals between each series were 30s. Frequency of execution was 3 days per week. The patient was also asked to perform stretching exercises for quadriceps and hamstring muscles, lasting 15s per muscle group, twice a day and 6 days which lasted a week. In order to increase adherence to the intervention, a daily control register was issued for the participant's exclusive use, in which he/she would record the exercises they performed on the corresponding days, the time it took to do them, and whether there were any adverse events. The KT was installed according to the manufacturer's specifications (Kinesio®), contained in the envelope in which the pre-cut product is sold. This was done during each follow-up visit during the study. Installation was accomplished by a single applier, which is certified by the manufacturing company for a basic course and declares no conflict of interest. The kinesiotape pre-cut knee tape pack contains 3 sections of tape: 2 black (I-strip and Y-strip) and 1 blue (I-strip) tape. With the knee flexed at 90°, the base of the black “I” strip was adhered on the leg midline about 15cm above the interarticular line (IAL). No tension was applied and the strip was spread over the same midline to about 5 –7.5cm below the IAL. The Y-strip was then applied, also without tension, and each tail extended to the sides of the midline. After applying the KT to each participant, generation of the “convolution” effect on the skin was confirmed, requesting the participants’ complete extension of both knees. The placebo technique was installed under the same conditions, on days different from those of the participants of the experimental group. The same material was used, but without the specifications contained in the envelope: a single black “I” strip with high tension (>50%) and while the knees were flexed at 90° with a bearing surface. applications were carried out by means of an unblinded applier, given the nature of the intervention. To maintain the sample blind, in each evaluation participants were asked to wear pants or long skirts to prevent them from showing the applied technique. Participants were given an appointment after 1 week to reinstall the corresponding tape, check the daily control register, and confirm permanence in or withdrawal from the study.
MeasurementsIn the first session, prior to application of the tape, the Visual Analog Scale (VAS) for pain intensity (0–10cm) and the WOMAC index were applied for baseline measurement. At the end of weeks 2, 4, and 6, the VAS and WOMAC were again applied. At the end of week 6, the notebook was reviewed and a final appointment was assigned to inform the participants of the results.
Statistical analysisOur hypothesis was that the group with strengthening exercise and KT would have 2 fewer points of difference in knee pain, compared with the control group, measured through the WOMAC pain subscale. With a α of a 0.05 and a β of 80%, we consider data published by Chang et al.9 to express a mean difference of 1.7 points for pain (Standard Deviation [SD]=0.9 and 1.5) and of 8.2 points for physical function (SD=4.8 and 8.3) of WOMAC subscales, a sample of 12 participants was calculated per group. The sample was increased by 20% to prevent losses, and two more participants were added to balance the groups for the performance of block randomization. N was 16 women per group.
Descriptive analysis of demographic variables was performed. Baseline comparisons were made with the Student's t test and the χ2 test and the correlation coefficient for pain was carried out by the VAS and the WOMAC index. On intergroup analysis, a Friedman test was used for related samples, calculation of percentage change for EVA and WOMAC and recalculation of Spearman's correlation coefficient between pain variables during the comparison of repeated measures. Intergroup comparison was conducted as follows: calculating analysis of covariance (general linear model) with Bonferroni statistic; Hotelling trace criterion to determine the significance of interaction between times (repeated measures) per treatment group; percentage of change for VAS and WOMAC (from the baseline value of the covariable corresponding to the baseline mean of both groups at week 6 of follow-up), and correlation coefficient between VAS and WOMAC variables during comparison of repeated measures and by interaction between assignment type and BMI category on percentage of change in pain. Analysis was performed by intention-to-treat. The software used was IBM SPSS Statistics for Windows (Version 23.0; IBM Corp., Armonk, NY, USA) Significance level was set at p≤0.05 throughout the study.
Ethical aspectsThis study took into account the principles of respect, beneficence, and justice, as well as international ethical guidelines with regard to recommendations for an additive design.27,28 The study was initiated once approval was obtained from the Institutional Review board and Ethics Committee. Informed consent was accepted and signed by each participant.
ResultsBaselineWe interviewed 39 subjects who fulfilled inclusion criteria. 7 of them were excluded by diverse conditions. In the control group, there were 2 voluntary dropouts (change of address and labor issues) and in the experimental group there were 4 (two reactions associated with the use of the KT but not with the materials – use of an external fixative substance and adhesive tape–, voluntary dropout for academic reasons and other due to mechanopostural low back pain). We followed up the corresponding cases (Fig. 1).

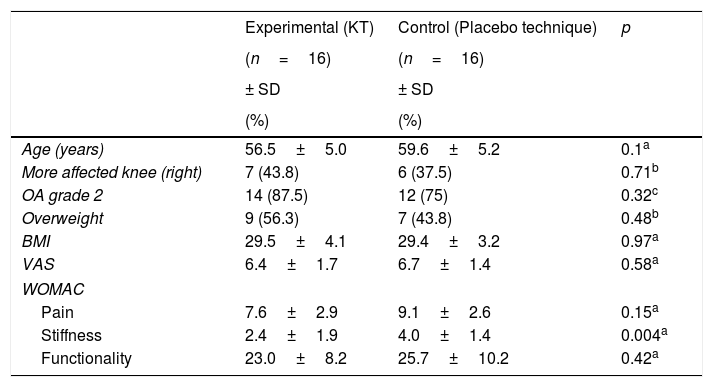
In the baseline state, there were no significant differences in demographic variables, but the allocation groups differed in terms of mean stiffness (p=0.004), with a higher score in the placebo group (Table 1). In this baseline data, as might be expected, pain measured by VAS and WOMAC correlated with a Pearson r coefficient of 0.445 (p=0.01); BMI correlated with physical function (r=0.400; p=0.02). Within WOMAC, pain with stiffness (r=0.553; p=0.001) and pain with physical function (r=0.601; p<0.001) also exhibited correlation. Finally, stiffness and physical function correlated with a coefficient of r=0.363 (p=0.04). Only physical function tended to be different according to the degree of obesity, with 27.3±9.9 points for participants with grade I and 21.5±7.6 points for those with overweight (p=0.07). The remaining variables (age, VAS, pain, and stiffness) were similar between patients with obesity and those with overweight (p>0.05). There was also no association between degrees of obesity and the affected knee (p=0.28) or with degree of OA (p=0.32), and the latter were not associated with each other (p=0.53). Baseline VAS was higher in cases in which the affected knee was the right one with 7.4±0.9 points vs. 6.0±1.6 with the left one (p=0.008); pain and stiffness. On the other hand, Baseline VAS also differed according to the degree of OA: grade 3 was more painful (10.6±8.3 points) than grade 2 with 7.8±2.5 points (p=0.02), and there was greater stiffness, with 4.5±2.2 points for grade 3 vs. 2.9±1.3 points for grade 2 (p=0.02).
Demographic and baseline values of the sample.
| Experimental (KT) | Control (Placebo technique) | p | |
|---|---|---|---|
| (n=16) | (n=16) | ||
| ± SD | ± SD | ||
| (%) | (%) | ||
| Age (years) | 56.5±5.0 | 59.6±5.2 | 0.1a |
| More affected knee (right) | 7 (43.8) | 6 (37.5) | 0.71b |
| OA grade 2 | 14 (87.5) | 12 (75) | 0.32c |
| Overweight | 9 (56.3) | 7 (43.8) | 0.48b |
| BMI | 29.5±4.1 | 29.4±3.2 | 0.97a |
| VAS | 6.4±1.7 | 6.7±1.4 | 0.58a |
| WOMAC | |||
| Pain | 7.6±2.9 | 9.1±2.6 | 0.15a |
| Stiffness | 2.4±1.9 | 4.0±1.4 | 0.004a |
| Functionality | 23.0±8.2 | 25.7±10.2 | 0.42a |
Distribution determined by Shapiro–Wilk.
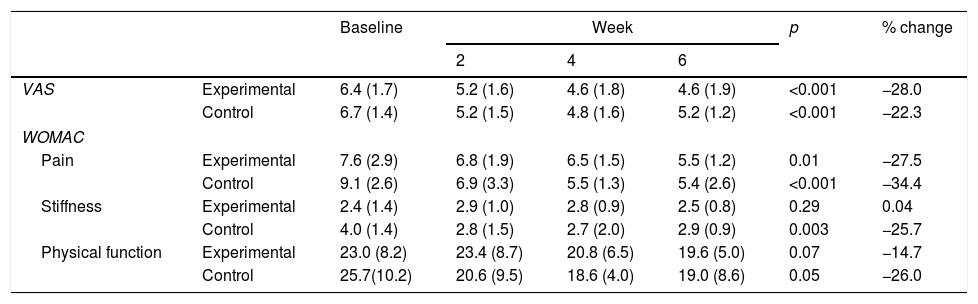
In the experimental group (Table 2), the VAS decreased from 6.4 to 4.6 (−28%) from baseline to week 6 (p<0.001), while pain decreased from 7.6 to 5.5 (−27.5%) during the same time period (p=0.01). There was no significant change in stiffness, and the physical function scale decreased −14.7% with respect to the baseline score (p=0.07). The percentage of change in pain correlated with percentages of change in stiffness (r=0.772; p<0.001) and physical function (r=0.693; p=0.003); therefore, as pain decreased, stiffness decreased and physical function improved. On the other hand, the change in pain and the decrease in stiffness correlated with a change in an increase in physical function (r=0.880; p=0.0001). In the placebo group (Table 2), VAS decreased from 6.7 to 5.2 (−22.3%) of the baseline value at week 6 (p=0.001), while pain decreased from 9.0 to 5.9 (−34.4%) during the same time period (p=0.0001); stiffness decreased from 4.0 to 2.9 (−25.7%) (p=0.003) and the functional scale was reduced by 26.0% (p=0.05). Similar to the correlations observed in the experimental group, in the control group, the percentage of change in pain correlated with the percentages of changes in stiffness (r=0.888; p<0.001) and in physical function (r=0.612; p=0.012), implying that, as pain decreased, stiffness decreased and functionality improved. In addition, the change in the decrease in stiffness correlated with a change in the increase of functionality (r=0.521; p=0.03).
Intragroup measures – experimental (KT) and control (Placebo technique).
| Baseline | Week | p | % change | ||||
|---|---|---|---|---|---|---|---|
| 2 | 4 | 6 | |||||
| VAS | Experimental | 6.4 (1.7) | 5.2 (1.6) | 4.6 (1.8) | 4.6 (1.9) | <0.001 | −28.0 |
| Control | 6.7 (1.4) | 5.2 (1.5) | 4.8 (1.6) | 5.2 (1.2) | <0.001 | −22.3 | |
| WOMAC | |||||||
| Pain | Experimental | 7.6 (2.9) | 6.8 (1.9) | 6.5 (1.5) | 5.5 (1.2) | 0.01 | −27.5 |
| Control | 9.1 (2.6) | 6.9 (3.3) | 5.5 (1.3) | 5.4 (2.6) | <0.001 | −34.4 | |
| Stiffness | Experimental | 2.4 (1.4) | 2.9 (1.0) | 2.8 (0.9) | 2.5 (0.8) | 0.29 | 0.04 |
| Control | 4.0 (1.4) | 2.8 (1.5) | 2.7 (2.0) | 2.9 (0.9) | 0.003 | −25.7 | |
| Physical function | Experimental | 23.0 (8.2) | 23.4 (8.7) | 20.8 (6.5) | 19.6 (5.0) | 0.07 | −14.7 |
| Control | 25.7(10.2) | 20.6 (9.5) | 18.6 (4.0) | 19.0 (8.6) | 0.05 | −26.0 | |
Friedman test, k-related groups.
The change percentage was calculated from the baseline value of the covariate, which corresponds to the baseline mean of both groups up to week 6 of follow-up. Respectively for placebo and experimental group, there was a difference of 8.2% improvement in the VAS (1.9 and 1.3 points, p=0.16), while for the subscales there were 1.1% for pain (2.7 points for both groups, p=0.2), 8.3% for stiffness (0.7 and 0.4 points, p=0.1) and 5% for physical function (4.5 and 5.7 points, p=0.65). None was significant. According to the Bonferroni test, no significant differences were observed in any of the measurements of weeks 2, 4 and 6, except for week 4 for the pain subscale (p=0.01) with a difference of 1.3 points and in week 2 for the stiffness subscale (p=0.04) with a difference of 0.9 points.
DiscussionAlthough KT is a widely used technique for the control of pain in several joint pathologies, in our study the use of KT was not associated with a significant improvement in the WOMAC scale when evaluating knee OA. The results obtained here indicate that quadriceps strengthening exercise accompanied by KT or a placebo technique decreases the pain measured by VAS and WOMAC after 6 weeks of treatment, by 27.5 and 34.4%, respectively. However, at the time of comparing the two interventions with each another by means of covariance analysis, the results exhibited a certain fluctuation, such as the difference in pain at week 4 and in stiffness at week 2 in the placebo technique group. However, there were not significant differences between them. In other words, it is equally effective to apply KT or to apply the placebo technique.
Specifically, we had negative results similar to authors like Wageck, Aydogdu and Kocygit.17–19 Wageck gives an intervention of only 4 days of in situ KT without taking into account the degree of OA, while Aydogdu is the only one that includes the exercise as part of the experiment and gives a 3-week intervention in a study where it is not clear if among the participants there was a method to avoid contamination between groups. In this study the number of exercise sessions is less than in our study and we consider that the presence of electrotherapy and cryotherapy makes the sum of effects more complex. Kocygit, on the other hand, measures effects of the KT after 12 days, with a continuous application every 4, which we think, is a more adequate way to maintain the effect that could have been enhanced by the exercise of having been applied. This author extends the age range from 30 to 70 years, which makes it difficult to determine if some participants had a greater degree of variability with respect to muscle condition and cartilage injury. In contrast, Akinbo, Anandkumar, Cho and Kaya20–23 have results contrary to ours in their studies. Akinbo finds important, but perhaps obvious, differences in favor of the population with knee injury due to sports activity, who will have a better response to pain due to their physical condition and age. Due to the inequality between the interventions and the characteristics of the groups, the value of their measurements is compromised and restricts the comparisons. With Anandkumar, the convolution effect seems to be responsible for an improvement in strength, but the taping techniques were very similar to each other. Probably varying the taping intervention would have differentiated the techniques and given more reliability to the measurements. Other drawbacks are that it does not indicate whether the measurements were made with or without the taping applied and that incorporates participants with OA grade I, in whom strength can be seen best expressed. Cho has very significant results in relation to pain and proprioceptive capacity and like the Anandkumar study; the convolution effect seems to be responsible for the improvement, since the tension seems to be large enough to eliminate this possible effect in the placebo. We think that if the number and size of convolutions is a factor to improve the effects on pain and strength, then somatotype and age are important, because skin folds can be formed more easily in the elderly and in ectomorphic subjects. Regarding Kaya, it presents pain improvement during the walk qualified with ALF score and degree of pain to the activity qualified with VAS. An important contribution is the application of KT on hamstring musculature, as other techniques suggest only applies to the quadriceps region. Related to this, it should be noted that there is a relationship of unilateral forces in the knee and that maintaining the best balance between the quadriceps and the hamstrings can give important clinical improvements. We found that other authors present their conclusions considering immediate measurements to the installation of the KT, include male and female population producing unbalanced categories, take into account grades 1 and 4 of OA and it is intended to award the KT short-term effects on a chronic injury that requires a treatment with proven effects, such as exercise.
In this study, we attempted to pay attention to the risk of having a high BMI and its possible consequences for pain as part of the secondary objectives; however, the results remained inconsistent, in that pain correlating with stiffness and physical function exhibited no decrease according to OA grade and overweight/obesity characteristics. Application of the placebo is very debatable under different circumstances as follows: if the material is of the same type, the effect is not clear of the tape's different tensions and extensions, in addition to the mechanisms involved at the neurobiological level that continue to be investigated. However, the intention of the study was to apply what was indicated by the creator and the manufacturer of the KT, which is to give rise to the convolution effect that increases the blood and lymphatic flow as well as the decompression of local pain receptors. In another study, Parreira29 reported similar results in a clinical trial with intervention for low back pain. In shoulder injuries, Kaya12 and Thelen13 also found improvements for each group that was associated with the application of therapeutic exercise, in the same manner and without differences between groups. In these cases, as in our experiment, the difference in the application of the tape present in both groups was the tension of the strips and the generation of the previously mentioned effect. We are in agreement in mentioning that this technique may not possess the manufacturer's stated vascular or nervous effect, which could be related to muscle activation, at least in these chronic injuries. This is similar to a study published by Lins,30 in which the authors experimented with variables of balance and strength at the electromyographic level without finding significant effects. Nonetheless, but it is noteworthy that their population comprised healthy women in which the differences may be more difficult to find and with measurements at the short term.
We consider that the duration of the exercise, the continuity in the application of the KT, the selection of grades 2 and 3 of OA and limiting the selection to women with a common BMI in this population are strengths of our study. Some limitations of our study are the non-determination of strength through objective methods such as isokinetic, as this would have verified the changes resulting from the training. As Cho did, we did not install tape on the hamstring muscles, which might have biomechanically favored the development of strength. Only verbal control was taken with regard to the intake of medications (only requesting that no NSAIDs or analgesics be taken during the duration of the intervention). We also think that it is likely that a third group, without taping and only with exercise, contributed with more data. Unfortunately, although a sample size was calculated, we believe that the number of measurements may have been reduced to apply parametric statistical analysis techniques. Finally, although an instruction session was given, the exercise prescription was carried out at home, so it was not supervised.
We can conclude that in our study, KT added to strengthening therapy does not offer a significant improvement in pain compared with quadriceps strengthening exercise alone in knee OA.
Conflict of interestsThe authors declare no conflict of interest.
The authors thank the following for his participation as statistical advisor Dr. Saúl Renán León Hernández. For their comments and help during academic sessions, Dr. María Eugenia Zghaib Rivero, Dr. Ailema J. González Ortíz, Dr. Rebeca Ramírez Morales and Dr. Fabiola López Bautista.


