





A 58 year old Caucasian women, with HLA-B27-positive mixed involvement spondyloarthritis (rachialgia and sacroiliac pain, both bilateral inflammatory with onset at the age of 21 currently with radiographic grade IV sacroiliitis associated with peripheral arthropathy of the small joints in the hands, ankles and metatarsophalanges with onset at the age of 55 years), in addition to previous repeated episodes of uveitis (4 episodes which abated with no sequelae), refractory to treatment with non-steroidal anti-inflammatory drugs, systemic corticoids at intermediate doses, methotrexate and leflunomide. In September 2015 treatment was initiated with golinmumab (anti-TNF alpha), resulting in a complete improvement of symptoms. The patient was symptom-free until July 2017 when she presented with symptoms compatible with linear localized morphea in lower limbs (Fig. 1) with no other concomitant infectious or neoplastic condition, confirmed by skin biopsy (fibrosing sclerodermiform dermatitis). This association in patients with immune-mediated diseases has been described but in highly exceptional cases. Following review of the literature, we found 6 similar cases, which are described in Table 1.1–6 We therefore believe that the presentation of morphea in a patient treated with anti-TNF alpha may be considered a possible condition associated with its use, even if presentation is not immediate and is infrequent, and that it should be taken into account by professionals who use these therapies.
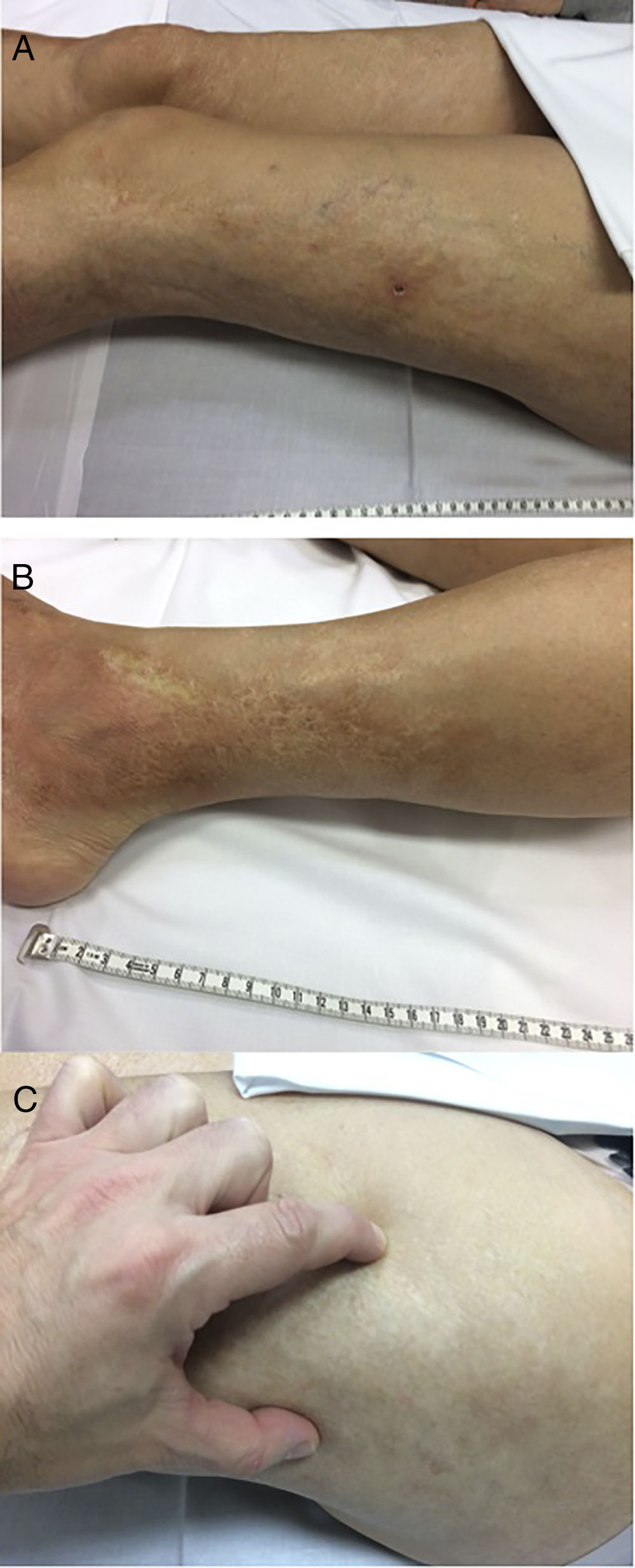
Multiple images of lower limb linear distribution indurated plaques, compatible with linear localised morphea: (A and B) sclerotic plaques with a pearly cream or whitish centre and violacious erythematous periphery, oedematous in lower left limb, compatible with active lesion; (C) image A lesion with demonstrable induration when pressed digitally; (D and E) extensive whitish scar-like plaques in the lower right limb, compatible with non active lesion.
Patient data with combined morphea and anti-TNF usage condition: review of the literature.
| Author | SexAgeRace | Anti-TNF alpha type | Interval from initiation of anti-TNF until beginning of morphea (weeks) | Immune-mediated disease | Distribution | Compatible Biopsy | Resolution after withdrawal of anti-TNF alpha (treatment) |
|---|---|---|---|---|---|---|---|
| Matozzi C, et al.1 | Woman17Caucasican | Adalimumab | 12 | Crohn | Abdomen (injection site) | Yes | Yes, complete (topical) |
| Stewart FA, et al.2 | Man45Caucasian | Etanercept | 78 | Psoriasis | Abdomen (injection site and trunk | Yes | Yes, with minimal progression (topical) |
| Ranganathan P3 | Woman52Afro-American | Infliximab | 14 | Rheumatoid arthritis | Neck, trunk, upper extremities | Not undertaken | Yes, partial (topical) |
| Ramírez J, et al.4 | Man37Caucasian | Adalimumab | 52 | Ankylosing spondylitis | Lower Extremities | Yes | Yes, partial (topical) |
| Inoue-Nishimoto T, et al.5 | Woman42Asian | Adalimumab | 26 | Psoriasis | Trunk and pelvic girdle | Yes | Yes, partial (topical) |
| Chimenti MS, et al.6 | Man54Caucasian | Etanercept | 156 | Rheumatoid arthritis | Trunk and abdomen | Yes | Yes, partial (rituximab) |
The authors have no conflict of interests to declare.
Please cite this article as: Torrente-Segarra V, Campo P, Heredia S, Heras-Mulero C, Bonet M. Morfea lineal asociada al uso de golimumab en paciente con espondiloartropatía. Reumatol Clin. 2020;16:303–305.


