









The Spanish Society of Rheumatology carried out the EPISER2000 study in 2000 to determine the prevalence of osteoarthritis and other rheumatic diseases in the Spanish population. Recent sociodemographic changes and lifestyle habits in Spain justified updating the epidemiological data on osteoarthritis and other rheumatic diseases (EPISER2016-study).
ObjectiveTo estimate the prevalence of symptomatic osteoarthritis of the cervical spine, lumbar spine, hip, knee and hand in the adult population in Spain.
Material and methodsCross-sectional population-based study. A multistage and stratified random cluster sampling was carried out. The participants were contacted by telephone to complete an osteoarthritis screening questionnaire. A rheumatologist confirmed or discarded the diagnosis. The ACR-clinical-criteria were used to diagnose hand-osteoarthritis and the ACR-clinical-radiological criteria to diagnose knee- and hip-osteoarthritis. To estimate the prevalence and its 95% confidence interval, weights were calculated according to the probability of selection in each of the sampling stages.
ResultsThe prevalence of osteoarthritis in Spain in one or more of the locations studied was 29.35%. The prevalence of cervical-osteoarthritis was 10.10% and of lumbar-osteoarthritis 15.52%. Both are more frequent in women and at older ages, as well as in people with low levels of education and obesity. The prevalence of hip-osteoarthritis was 5.13%, that of knee-osteoarthritis 13.83%, these are associated with female sex, overweight and obesity. The prevalence of hand osteoarthritis was 7.73%. It is more frequent in women, who are obese, with a low educational level and who are older.
ConclusionThe EPISER2016 study is the first to analyse the prevalence of symptomatic osteoarthritis in 5 locations (cervical, lumbar, knee, hip and hands) in Spain. Lumbar spine osteoarthritis is the most prevalent.
La Sociedad Española de Reumatología elaboró en el año 2000 el estudio EPISER2000 para conocer la prevalencia de la artrosis y otras enfermedades reumáticas en España. Los cambios sociodemográficos y en los hábitos de vida ocurridos en los últimos años en España justifican actualizar los datos de las enfermedades reumáticas (EPISER2016).
ObjetivoEstimar la prevalencia de artrosis sintomática de columna cervical, columna lumbar, cadera, rodilla y mano, en población adulta en España.
Material y métodosEstudio transversal de base poblacional. Se realizó un muestreo aleatorizado polietápico estratificado y por conglomerados. Los participantes fueron contactados por teléfono para cumplimentar un cuestionario de cribado de artrosis. El reumatólogo confirmaba o descartaba el diagnóstico. Se utilizaron los criterios-clínicos-ACR para diagnosticar artrosis de manos y los criterios clínico-radiológicos-ACR para diagnosticar la artrosis de rodilla y cadera.
ResultadosLa prevalencia de artrosis en España en una o más de las localizaciones estudiadas fue de 29,35%. La prevalencia de artrosis-cervical fue del 10,10% y de artrosis-lumbar del 15,52%. Ambas son más frecuentes en mujeres y a mayor edad, así como en personas con niveles de estudios bajos y obesidad. La prevalencia de artrosis de cadera fue del 5,13% y la de artrosis de rodilla del 13,83%; estas se asocian con el sexo femenino, sobrepeso y obesidad, menor frecuencia en nivel de estudios alto y con la edad. La prevalencia de la artrosis de mano fue del 7,73%. Es más frecuente en mujeres, obesas, con bajo nivel de estudios y mayor edad.
ConclusionesEl estudio EPISER2016 es el primero que analiza la prevalencia de artrosis sintomática en 5 localizaciones (columna cervical, lumbar, rodilla, cadera y manos) en España. La artrosis de la columna lumbar es la más prevalente.
Arthrosis cannot be described as a single disease, but rather as a heterogeneous group of diseases with similar clinical manifestations involving common pathological and radiological changes. The OARSI recently defined arthrosis as a disorder which affects the mobile joints that is characterised by cellular stress and degradation of the extracellular cartilage matrix and commences with micro- and macrolesions which activates poorly adapted repair responses, including innate immunity pro-inflammatory routes. The disease manifests firstly as a molecular alteration (abnormal joint tissue metabolism), followed by anatomical or physiological alterations (characterised by cartilage degradation, bone remodelling, joint inflammation and loss of normal joint function), which may culminate in the emergence of the disease.1
Arthrosis is considered to be the most common rheumatological disease; nevertheless, epidemiological studies sometimes show different results. These differences are largely due to the definition of patients with arthrosis. Due to this it is important when interpreting epidemiological data to know whether the studies in question have defined cases as symptomatic or radiological arthrosis.2
Three cross-sectional studies have been published in Spain which calculate the prevalence of arthrosis. The first of these, which was published in 1982, was based on a study undertaken in the town of Los Cortijos (Ciudad Real). A total of 827 individuals were analysed, 87% of the selected population, by means of their clinical history, physical examination, analysis and radiological study. 20% of the population were over the age of 60 years old. 26.1% suffered arthrosis.3 The second study was undertaken in Asturias and published in 1993. 702 individuals over the age of 18 years were evaluated, 76% of the invited population, selected by randomised, stratified, multistage and proportional sampling. All of the subjects were interviewed by trained doctors, and validated criteria were applied to establish the diagnoses. 23.8% of the sample was diagnosed with arthrosis.4 The third study was EPISER2000, promoted by the Sociedad Española de Reumatología, with subjects over the age of 20 years. It estimated that the prevalence of symptomatic knee arthrosis in Spain stood at 10.2% and that of the hands at 6.2%.5,6 It has to be underlined that EPISER2000 did not analyse the prevalence of axial arthrosis.
Sociodemographic and lifestyle changes over recent years in Spain justify updating the epidemiological data corresponding to arthrosis.7 The sociodemographic changes can be summarised as an increase in the proportion of individuals over the age of 64 years and an increase in the percentage of foreign population, according to Instituto Nacional de Estadística data.8 Regarding lifestyle changes, an increase in obesity and overweight individuals has been observed, together with changes in tobacco consumption.9–11
The main aim of the EPISER2016 study, which was promoted by the Sociedad Española de Reumatología, was to estimate the prevalence of the main rheumatic diseases within the adult population in Spain. These diseases include arthrosis in the locations already included in EPISER2000 (the hip, knee and hand) and this update expands to include the cervical and lumbar spinal column. As a secondary objective its associations with sociodemographic, anthropometric and lifestyle variables have also been examined.
Material and methodsThe methodology and sample characteristics of the EPISER2016 study have been described before.7,12 To summarise, it is a cross-sectional study of a population base. Multi-stage stratified and grouped sampling was used. Subjects who live in 78 towns of 17 autonomous communities took part, within the catchment area of 21 hospitals (Fig. 1). Given the size of the sample and the limited magnitude of the differences respecting the general population for the characteristics that were analysed, the sample finally included in EPISER2016 could be considered to be representative of the general adult population of Spain for the estimation of the prevalence of rheumatic diseases. The sample included in the arthrosis prevalence study was composed of 3336 individuals aged 40 years and above.

Hospitals and towns which took part in each one of the participating autonomous communities: Hospital General Universitario de Elda: Cañada, Algueña, Sax, Beneixama, Biar, El Pinós, Salinas, Hondón de los Frailes, Hondón de las Nieves (Comunidad Valenciana). Hospital General de Ontinyent: Fontanars del Aforins, Atzeneta D’Albaida, Bocairent, Agullent, Aielo de Malferit, Albaida, Bèlgida, Palomar, Benisoda, Carricola, Bufalí (Comunidad Valenciana). Complejo Asistencial Universitario de Palencia: Torquemada, Baltanás, Paredes de Nava, Dueñas, Villada, Herrera de Pisuerga, Carrión de los Condes, Saldaña, Osorno (Castilla y León). Hospital Comarcal de Monforte de Lemos: Quiroga, Carballedo, Folgoso do Courel, Chantada, Bóveda, Saviñao, Sober, Pantón (Galicia). Complejo Hospitalario de Navarra: Lekunberri, Aoiz, Mendigorria, Sangüesa, Olite, Irurtzun, Puente de la Reina, Larraga, Falces (Navarre). Hospital Universitario Puerta del Mar: San Fernando, Cádiz (Andalusia). Complejo Hospitalario Universitario de Jaén: Martos, Jaén (Andalusia). Hospital Universitario Central de Asturias: Langreo, Oviedo (Asturias). Hospital de Barbastro: Barbastro, Monzón (Aragón). Hospital Comarcal de Inca: Inca, Sa Pobla (Balearic Islands). Hospital Universitario Nuestra Señora de la Candelaria: Güimar, Candelaria (Canary Islands). Hospital Universitario Marqués de Valdecilla: Camargo, Santander (Cantabria). Complejo Hospitalario Mancha Centro: Campo de Criptana, Alcázar de San Juan (Castilla La Mancha). Hospital Universitario Germans Trias i Pujol: El Masnou, Santa Coloma de Gramenet, Sant Adriá del Besós (Catalonia). Hospital Universitari Parc Taulí: Barberà de Vallès, Sabadell (Catalonia). Hospital de Mérida: Mérida, Almendralejo, Montijo (Extremadura). Fundación Hospital de Calahorra: Calahorra, Arnedo (La Rioja). Hospital Universitario Severo Ochoa: Leganés (Madrid). Hospital El Escorial: San Lorenzo de El Escorial, Galapagar (Madrid). Hospital Rafael Méndez: Águilas, Lorca (Murcia). Hospital Universitario de Cruces: Sestao, Baracaldo (Basque Country).
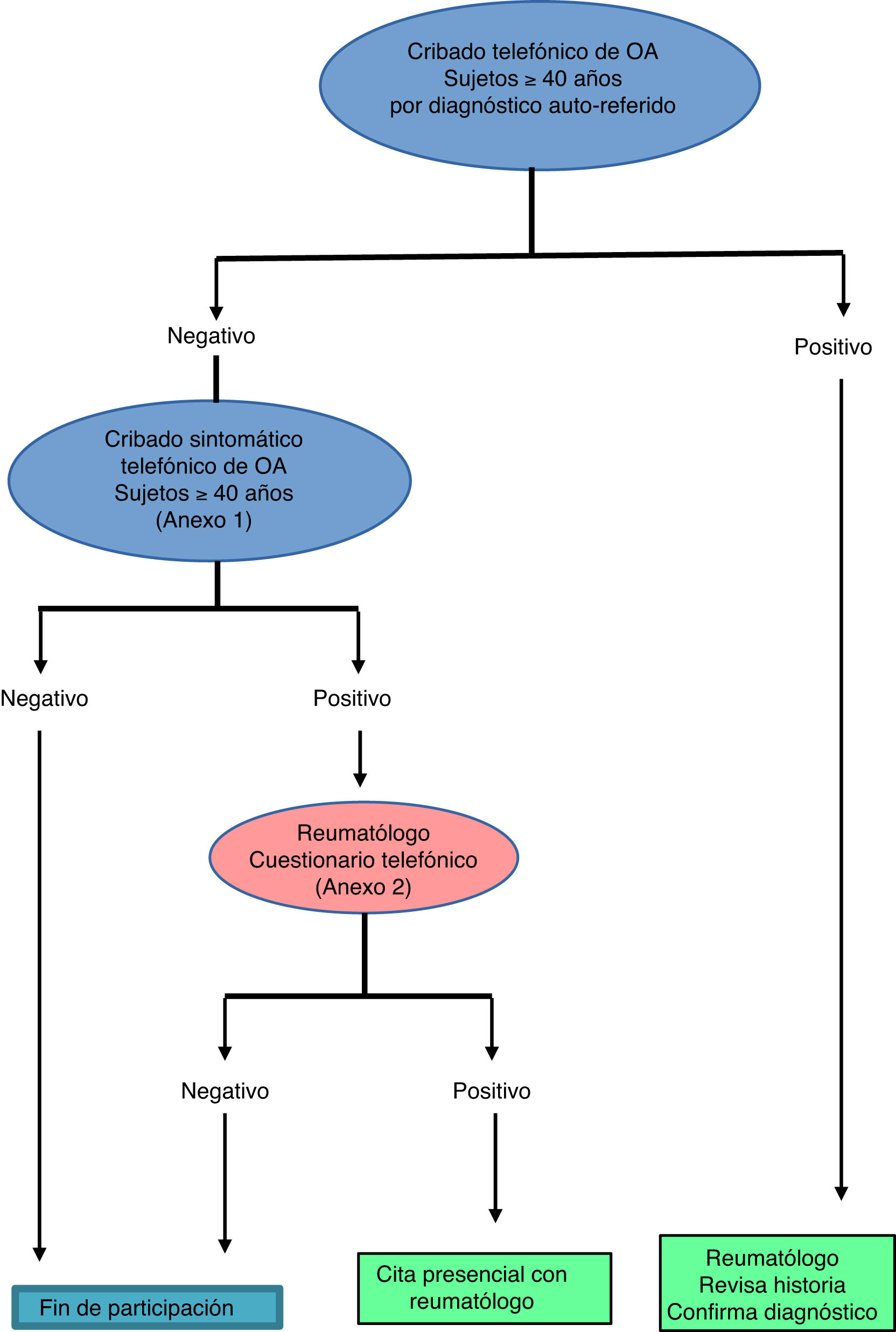
Interviewers in a call centre screened the sample using a telephonic questionnaire that covered two complementary routes: self-diagnosis and screening according to symptoms (Fig. 2, Appendix A, annex 1). If the patients stated that they had already been diagnosed, a rheumatologist subsequently confirmed their diagnosis by reviewing their clinical history. The patients who had no previous diagnosis, based on their replies to the symptom-based screening, either fulfilled the criteria for suspicion or did not. If they did not fulfil these criteria, their participation in the study was terminated. If they did fulfil the criteria, the next step consisted of a rheumatologist applying another more specific telephonic questionnaire (Appendix A, annex 2) to select the individuals with a persistent suspicion of diagnosis of arthrosis. These patients were given an appointment with the rheumatologist for a physical and radiological examination, to definitively confirm or rule out the diagnosis.
Cases were considered to have been lost when the subject completed the initial telephonic questionnaire with a positive result in the screening for arthrosis and the rheumatologist was unable to confirm or rule out the diagnosis.
All of the subjects were asked to give their informed consent orally in the first telephonic contact. This was also requested in writing from those participants who visited the surgery for physical examination and complementary tests. The study was approved by the Research Ethics Committee of the Hospital Universitario de Canarias, which acted as the reference committee, and it was also approved by the research ethics committees of the participating hospitals when this was required.
Case definition (for the symptom-based screening process)The flow to define the case in one of the locations was as follows:
Cervical spinal column arthrosisGiven the lack of criteria defined by a scientific society for the diagnosis of axial arthrosis (cervical and lumbar spinal column), a member of the scientific committee who specialises in arthrosis (FJB) set the criteria used in this study. They were accepted by the chief researcher and the other members of the scientific committee.
Symptom-based screening: this was considered positive if the individual had had cervical pain that was not due to trauma or over-exertion during at least 3 months (even when the intensity of the pain varied) and it was exacerbated by neck movements.
Sustained suspicion: the individual was questioned once again to confirm the characteristics of the pain described in the screening section. If they were present, they were asked if a radiological study had been performed, and if so, about the results of the same. The suspicion was maintained if the individual mentioned pain with the characteristics described in the radiological study with abnormal results in the X-ray, or without the said study.
Confirmation of diagnosis: no criteria have been approved by a scientific society or group for this disease, so that the following criteria were defined specifically for this study:
- 1.
Cervical mechanical pain that evolved over more than 3 months.
- 2.
Rigidity for at least 30min or the absence of rigidity.
- 3.
Vertebral osteophytes or reduction of the intervertebral space, with plate sclerosis.
- 4.
Facet joint sclerosis.
The diagnosis was confirmed if both clinical criteria (1 and 2) were fulfilled, together with at least one of the radiological criteria (3 and 4).
Lumbar spinal column arthrosisSymptom-based screening: this was considered positive had had lumbar pain that was not due to trauma or over-exertion during at least 3 months (even when the intensity of the pain varied) and that it was exacerbated by picking up weight or making an effort.
Sustained suspicion: the individual was questioned once again to confirm the characteristics of the pain described in the screening section. If they were present, they were asked if a radiological study had been performed, and if so, about the results of the same. The suspicion was maintained if the individual mentioned pain with the characteristics described in the radiological study and the abnormal results in the X-ray, or without the said study.
Confirmation of diagnosis: no criteria have been approved by a scientific society or group for this disease, so that the following criteria were defined specifically for this study:
- 1.
Lumbar mechanical pain that had evolved over more than 3 months.
- 2.
Rigidity lasting at least 30min or the absence of rigidity.
- 3.
Vertebral osteophytes or a reduction of the space between vertebras with plate sclerosis.
- 4.
Facet joint sclerosis.
The diagnosis was confirmed if both clinical criteria (1 and 2) were confirmed, together with at least one of the radiological criteria (3 and 4).
Hip arthrosisSymptom-based screening: this was considered positive if the individual mentioned hip or groin pain that was not caused by trauma or over-exertion and lasted for more than 4 weeks, being exacerbated by effort, walking or going up or down stairs.
Sustained suspicion: the suspicion was maintained if the individual mentioned pain with the described characteristics and an abnormal result in a previous X-ray image, or without an X-ray image.
Confirmation of diagnosis: the clinical and radiological criteria of the ACR were used.13
Knee arthrosisSymptom-based screening: this was considered positive if the individual mentioned knee pain that was not caused by trauma or over-exertion and that lasted more than 4 weeks, becoming exacerbated by effort, walking or going up or down stairs.
Sustained suspicion: the suspicion was maintained if the individual mentioned pain with the described characteristics and an abnormal result in a previous X-ray image, or without an X-ray image.
Confirmation of diagnosis: ACR clinical and radiological criteria used as well as the clinical criteria.14 The clinical criteria were the same as the ones used in EPISER2000.
Hand arthrosisSymptom-based screening: this was considered positive if the individual mentioned hand pain that was not caused by trauma or over-exertion and that lasted for more than 4 weeks, became worse with use of the hands or finger movement.
Sustained suspicion: the suspicion was maintained if the individual mentioned pain with the described characteristics and an abnormal result in a previous X-ray image, or without an X-ray image.
Confirmation of diagnosis: The clinical criteria of the ACR were used,15 the same ones that were also used in EPISER2000.
Statistical analysisSample design was taken into account to calculate prevalence and its corresponding 95% confidence interval, and weightings were calculated according to the probability of selection in each one of the sampling stages, based on population distribution in Spain according to registration data of the Instituto Nacional de Estadística. This weighting was performed considering participants’ age, sex and geographical origin (three zones were defined: North [Galicia+Asturias+Cantabria+Basque Country+Navarre+La Rioja], Mediterranean and Canary Islands [Catalonia+Comunidad Valenciana+Balearic Islands+Murcia+Andalusia+the Canary Islands] and the Centre [Comunidad de Madrid+Castilla y León+Aragon+Castile-La Mancha+Extremadura]).
Lastly, predictive models were designed to analyse which of the sociodemographic, anthropometric and lifestyle variables included in the telephonic questionnaire were associated with each one of the diseases included in EPISER2016. To do this, bivariant analysis of the association of disease with each variable was first calculated, followed by the construction of binary logistic regression models based on the variables with a value of P<.2 in the bivariant analysis (age and sex were included in the model, regardless of the value of P in the bivariant). Associations where P<.05 were considered to be statistically significant. To compare different areas in Spain it was decided to use the North as the reference category, as in the majority of the multivariant analyses of the different locations of arthrosis it was found that this was the category with the lowest rates of the disease. V22 of the IBM SPSS Statistics program was used for analysis.
ResultsThe prevalence of symptomatic arthrosis in Spain, in one or more of the locations studied (cervical and lumbar spinal column, hips, knees or hands), amounted to 29.35% (CI 95%: 27.77–30.97) and it increased with age, reaching its highest figures in subjects over the age of 80 years (52.6%; CI 95%: 46.97–58.29). It was more common in women, above all those over the age of 60 years (Fig. 3).
Cervical spinal column arthrosis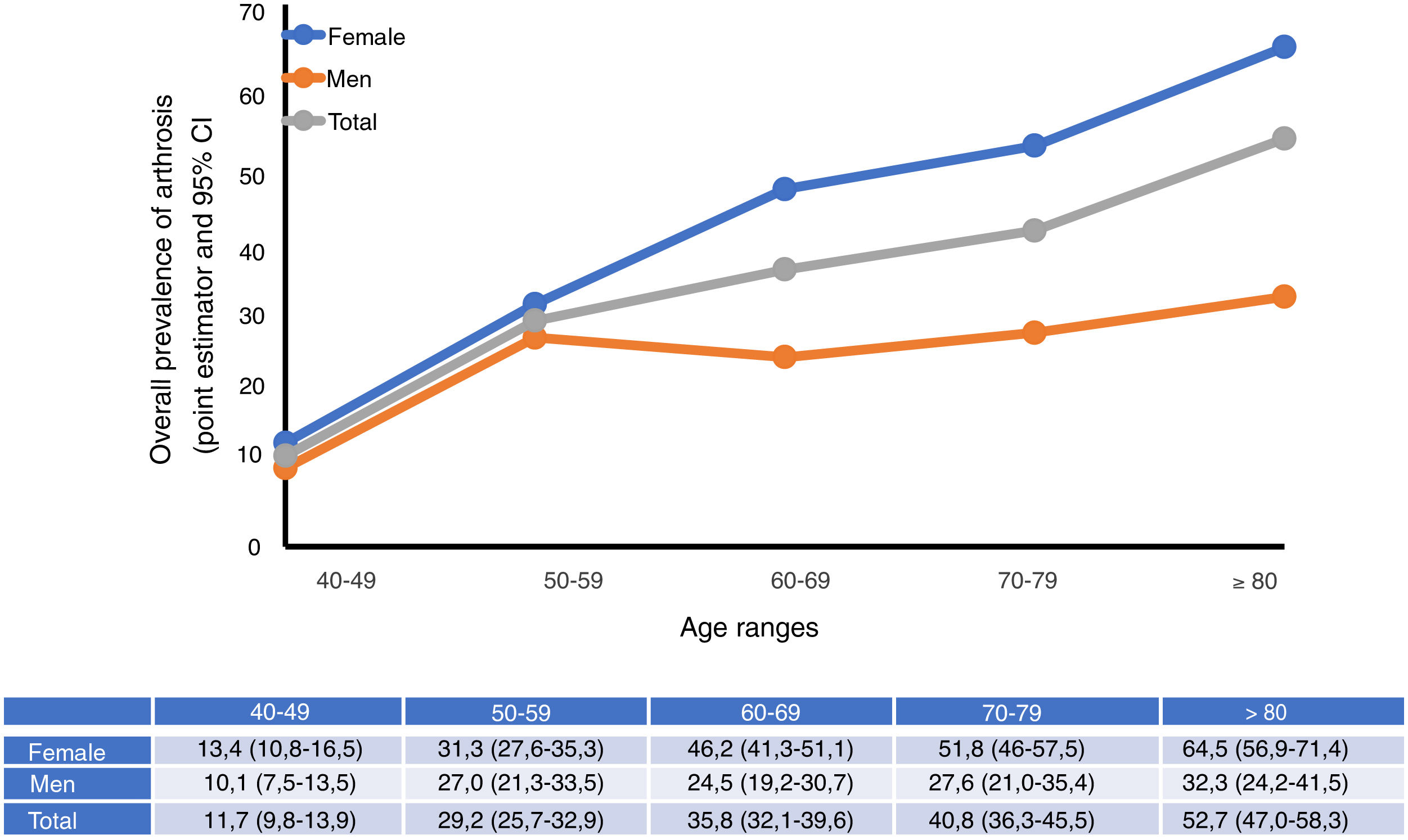
613 subjects screened positively for cervical arthrosis after the initial interview, and 28 of these were lost. The prevalence of cervical arthrosis was 10.10% (CI 95%: 9.07–11.24). In 93.33% (322/345) of cases the diagnosis was clinical – radiographical, and 78.26% (270/345) had been diagnosed prior to the study. The negative predictive value (NPV) of the complete call centre questionnaire (in its totality) in screening for cervical arthrosis was 99.19% (one case of the 123 subjects aged 40 or more years who were selected at random from the participants who had obtained a negative screening result for all of the diseases studied in EPISER2016).
Cervical arthrosis was associated in a statistically significant way with age, age, educational level, obesity and zone in Spain (Table 1). It was more frequent in women and at older ages (with prevalence peaking from 60 to 69 years old), and in cases of obesity and basic educational levels. Regarding the geographical area in Spain, cervical arthrosis was less common in the subjects in the north than it was in those in the Mediterranean area (+the Canary Islands) and the centre of Spain. Tobacco consumption, living in a rural or urban environment and having been born abroad were not associated with cervical arthrosis.
Variables associated with the presence of cervical arthrosis. Multivariant analysis.
| Variables | P | OR | CI 95% | |
|---|---|---|---|---|
| Lower | Higher | |||
| Age | ||||
| 40–49a | ||||
| 50–59 | <.001 | 2.047 | 1.387 | 3.022 |
| 60–69 | <.001 | 3.347 | 2.270 | 4.934 |
| 70–79 | <.001 | 2.337 | 1.495 | 3.654 |
| 80 or older | <.001 | 2.916 | 1.751 | 4.854 |
| Sex | ||||
| Female | <.001 | 2.241 | 1.660 | 3.025 |
| Educational level | ||||
| Primarya | ||||
| Secondary | .009 | .659 | .481 | .902 |
| Higher | <.001 | .431 | .304 | .613 |
| BMI | ||||
| Normal weighta | ||||
| Low weight | .840 | .857 | .192 | 3.821 |
| Overweight | .208 | 1.197 | .905 | 1.584 |
| Obesity | .002 | 1.679 | 1.209 | 2.332 |
| Region of Spain | ||||
| Northa | ||||
| Mediterranean (+Canarias) | .013 | 1.486 | 1.089 | 2.029 |
| Centre | .007 | 1.565 | 1.132 | 2.163 |
| Born abroad | .808 | .923 | .483 | 1.764 |
| Tobacco consumption | ||||
| Does not smoke and has never smoked habituallya | ||||
| Does not smoke now, but used to in the past | .169 | .809 | .598 | 1.094 |
| Yes, smokes every day | .344 | 1.177 | .840 | 1.650 |
| Yes, smokes but not every day | .504 | .664 | .200 | 2.206 |
777 subjects screened positively for lumbar arthrosis after the first interview, of which 31 were lost. The prevalence of lumbar spinal column arthrosis amounted to 15.52% (CI 95%: 14.30–16.83). Diagnosis was clinical – radiological in 97.59% (527/540) of cases, and 80.56% (435/540) were diagnosed prior to EPISER. The NPV of the complete call centre questionnaire (in its totality) was lumbar arthrosis screening was 98.37% (2 cases of the 123 subjects aged 40 years or more who took part in the NPV study).
As was the case for cervical spinal column arthrosis, lumbar spinal column arthrosis was more frequent in women, at an older age (with a peak in prevalence at ≥80 years), low educational levels and obesity (the association is stronger than was the case with cervical arthrosis and an association was also found with being overweight) (Table 2). In terms of geographical area, lumbar arthrosis was more common in the centre of Spain. Tobacco consumption, living in a rural or urban environment or having been born abroad were not associated with lumbar arthrosis.
Variables associated with the presence of lumbar arthrosis. Multivariant analysis.
| Variables | P | OR | CI 95% | |
|---|---|---|---|---|
| Lower | Higher | |||
| Age | ||||
| 40–49a | ||||
| 50–59 | <.001 | 2.000 | 1.438 | 2.781 |
| 60–69 | <.001 | 3.228 | 2.319 | 4.494 |
| 70–79 | <.001 | 3.200 | 2.223 | 4.607 |
| 80 or older | <.001 | 4.049 | 2.667 | 6.148 |
| Sex | ||||
| Female | <.001 | 2.324 | 1.816 | 2.973 |
| Educational level | ||||
| Primarya | ||||
| Secondary | .071 | .788 | .609 | 1.020 |
| Higher | <.001 | .433 | .322 | .583 |
| BMI | ||||
| Normal weighta | ||||
| Low weight | .998 | <.001 | <.001 | |
| Overweight | .001 | 1.528 | 1.201 | 1.945 |
| Obesity | <.001 | 2.490 | 1.881 | 3.295 |
| Region of Spain | ||||
| Northa | ||||
| Mediterranean (+Canary Islands) | .161 | .832 | .643 | 1.076 |
| Centre | .036 | 1.322 | 1.019 | 1.716 |
| Rural/urban | ||||
| Rural | .149 | 1.204 | .936 | 1.550 |
| Tobacco consumption | ||||
| Does not smoke and has never smoked habituallya | ||||
| Does not smoke now, but used to in the past | .119 | .820 | .638 | 1.052 |
| Yes, smokes every day | .565 | .914 | .674 | 1.241 |
| Yes, smokes but not every day | .832 | 1.095 | .473 | 2.534 |
396 subjects screened positively for hip arthrosis after the first interview, of which 6 were lost. The prevalence of hip arthrosis was 5.13% (CI 95%: 4.40–5.99). In 95.21% (158/166) of cases the diagnosis was clinical – radiological and 91.57% (152/166) of these subjects had been diagnosed prior to the EPISER study. The NPV of the complete call centre questionnaire (in its totality) for hip arthrosis screening was 100%.
Being overweight or obese were the factors that were associated with hip arthrosis, together with educational level and age (Table 3). The peak of prevalence was detected in subjects aged ≥80 years. A high educational level was associated with a lower frequency of hip arthrosis. An association at the limit of statistical significance was found for sex, with a higher frequency in women. Tobacco consumption, geographical area in Spain, having been born abroad and living in a rural or urban environment showed no association with the condition.
Variables associated with the presence of hip arthrosis. Multivariant analysis.
| Variables | P | OR | CI 95% | |
|---|---|---|---|---|
| Lower | Higher | |||
| Age | ||||
| 40–49a | ||||
| 50–59 | .278 | 1.473 | .732 | 2.966 |
| 60–69 | <.001 | 3.548 | 1.878 | 6.703 |
| 70–79 | <.001 | 4.374 | 2.248 | 8.513 |
| 80 or older | <.001 | 9.033 | 4.580 | 17.816 |
| Sex | ||||
| Female | .057 | 1.484 | .988 | 2.229 |
| BMI | ||||
| Normal weighta | ||||
| Low weight | .689 | 1.529 | .191 | 12.267 |
| Overweight | .017 | 1.668 | 1.094 | 2.544 |
| Obesity | .006 | 1.982 | 1.220 | 3.218 |
| Educational level | ||||
| Primarya | ||||
| Secondary | .313 | .793 | .506 | 1.244 |
| Higher | .001 | .383 | .216 | .680 |
| Tobacco consumption | ||||
| Does not smoke and has never smoked habituallya | ||||
| Does not smoke now, but used to in the past | .471 | .854 | .556 | 1.311 |
| Yes, smokes | .673 | .887 | .507 | 1.550 |
649 subjects screened positively for knee arthrosis after the first interview, of which 15 were lost. The prevalence of knee arthrosis was 13.83% (CI 95%: 12.66–15.11). Diagnosis was clinical – radiological in 92.48% (418/452) of cases, and 88.27% (399/452) had been diagnosed prior to the EPISER study. The NPV of the complete call centre questionnaire (in its totality) for knee arthrosis screening amounted to 95.12% (6/123).
The factors associated with knee arthrosis were sex (as it was more common in women), being overweight and obese, educational level (as it was less frequent in subjects with a high educational level) and age (prevalence was found to peak at over 70 years old) (Table 4). Prevalence in the Mediterranean area (+the Canary Islands) and living in a rural or urban environment were found to be associated with the condition to a degree that was close to being statistically significant. No association was found with tobacco consumption or having been born abroad.
Variables associated with the presence of knee arthrosis. Multivariant analysis.
| Variables | P | OR | CI 95% | |
|---|---|---|---|---|
| Lower | Higher | |||
| Age | ||||
| 40–49a | ||||
| 50–59 | <.001 | 2.934 | 1.864 | 4.620 |
| 60–69 | <.001 | 6.487 | 4.168 | 10.096 |
| 70–79 | <.001 | 9.568 | 6.039 | 15.157 |
| 80 or older | <.001 | 10.210 | 6.132 | 17.000 |
| Sex | ||||
| Female | <.001 | 2.008 | 1.531 | 2.633 |
| BMI | ||||
| Normal weighta | ||||
| Low weight | .998 | <.001 | <.001 | |
| Overweight | <.001 | 2.248 | 1.682 | 3.005 |
| Obesity | <.001 | 4.845 | 3.517 | 6.675 |
| Educational level | ||||
| Primarya | ||||
| Secondary | .162 | .809 | .601 | 1.088 |
| Higher | .001 | .573 | .414 | .793 |
| Tobacco consumption | ||||
| Does not smoke and has never smoked habituallya | ||||
| Does not smoke now, but used to in the past | .338 | .872 | .659 | 1.154 |
| Yes, smokes | .965 | .992 | .699 | 1.407 |
| Born abroad | .889 | 1.046 | .555 | 1.971 |
| Rural/urban | ||||
| Rural | .094 | .782 | .586 | 1.043 |
| Region of Spain | ||||
| Northa | ||||
| Mediterranean (+Canary Islands) | .073 | 1.301 | .975 | 1.734 |
| Centre | .188 | 1.228 | .905 | 1.667 |
488 subjects screened positively for hand arthrosis after the initial interview, of whom 12 were lost. The prevalence of hand arthrosis amounted to 7.73% (CI 95%: 6.89–8.67). 81.52% (225/276) of cases had been diagnosed prior to the EPISER study. The NPV of the complete call centre questionnaire (in its totality) for hand arthrosis screening was 97.56% (3/123).
The factors associated with hand arthrosis were sex, age, educational level and obesity. Hand arthrosis was more common in women and subjects who were obese, with a low educational level and older; the peak stood at ≥80 years. No association was found between tobacco consumption, region of Spain, having been born abroad and living in a rural or urban environment and hand arthrosis (Table 5).
Variables associated with the presence of hand arthrosis. Multivariant analysis.
| Variables | P | OR | CI 95% | |
|---|---|---|---|---|
| Lower | Higher | |||
| Age | ||||
| 40–49a | ||||
| 50–59 | <.001 | 4.005 | 2.339 | 6.857 |
| 60–69 | <.001 | 6.851 | 3.995 | 11.746 |
| 70–79 | <.001 | 6.425 | 3.600 | 11.470 |
| 80 or older | <.001 | 9.907 | 5.314 | 18.471 |
| Sex | ||||
| Female | <.001 | 3.369 | 2.333 | 4.864 |
| BMI | ||||
| Normal weighta | ||||
| Low weight | .598 | .575 | .074 | 4.491 |
| Overweight | .917 | .983 | .717 | 1.348 |
| Obesity | .003 | 1.698 | 1.190 | 2.423 |
| Educational level | ||||
| Primarya | ||||
| Secondary | .825 | .962 | .685 | 1.353 |
| Higher | .025 | .643 | .437 | .946 |
| Tobacco consumption | ||||
| Does not smoke and has never smoked habituallya | ||||
| Does not smoke now, but used to in the past | .233 | 1.220 | .880 | 1.693 |
| Yes, smokes | .498 | 1.150 | .767 | 1.725 |
The figures expressing the prevalence of arthrosis in the EPISER2016 study are generally higher than those corresponding to EPISER2000 (hands: 7.73% vs 6.2%; knees: 13.83% vs 10.2%). Nevertheless, when interpreting and comparing these results it is necessary to take into account the fact that the EPISER2016 study analysed the prevalence of arthrosis in the population ≥40 years old, while the EPISER2000 study did so for the population ≥20 years old.5
Another factor that has to be taken into account when comparing data is whether the studies defined cases as symptomatic or radiological arthrosis.2 Respecting this, the EPISER2000 study took symptomatic arthrosis into account for the hands and knees, as defined by ACR clinical criteria. In the EPISER2016 study, clinical and radiological criteria were used as well as the criteria used in EPISER2000 to diagnose knee arthrosis. The clinical criteria used in EPISER2000 were maintained for hand arthrosis.
An important novelty of EPISER2016 is the inclusion of spinal column arthrosis, giving rise to the first data on the prevalence of this condition in Spain. It is common in the population, in the cervical as well as the lumbar region. Few published works analyse the prevalence of axial arthrosis.16 Together with this lack of studies, there are also no validated criteria for the diagnosis of arthrosis in this location, so that we have been obliged to define them by combining clinical and radiological variables. These criteria were used to confirm suspicion in those cases that had not been diagnosed prior to the study.
EPISER2016 data support many of the known factors associated with arthrosis.17,18 Obesity is one of the most important of these factors. Many studies corroborate the association between obesity and arthrosis of the knees, hips and hands. The risk of suffering arthrosis is calculated to be 4 times higher in case of obesity for women and 4.8 times higher for men. EPISER2016 also shows an association with cervical and lumbar spinal column arthrosis. The causal mechanisms that would explain this associated have yet to be elucidated. A biomechanical cause would clearly not explain the association with hand or cervical spinal column arthrosis. The influence of metabolic factors in the pathogenesis of arthrosis is becoming increasingly relevant, underlining the existence of a metabolic phenotype for arthrosis.19
As is the case for obesity, sex and age are both factors which this study found to be associated with arthrosis in the 5 locations analysed. It occurs more frequently in women, and increased age seems to be more important factors for arthrosis of the lower limbs.
The association between tobacco consumption and arthrosis is under discussion: some studies, above all epidemiological ones, find tobacco use to be a protective factor, while others do not find any such association. In a 2017 systematic review and meta-analysis, the authors state that there is an inverse relationship between smoking cigarettes and the risk of knee arthrosis, chiefly in men. However, to date it has not been possible to find an explanation for this association, so that it has been suggested that more studies should be designed.20 Bivariant analysis in the EPISER2016 study shows a significant association between tobacco consumption and arthrosis in all of the locations studied, although this relationship does not emerge in the multivariant study.
The EPISER2016 study does not analyse the influence of occupation or work, although both factors were found by the NHANES-I and Framingham studies to contribute to the risk of arthrosis, above all of the knees, in professions that involve frequent use of the same, especially in bending (builders, firemen and sailors).17,18,21 Nevertheless, the EPISER2016 study includes educational level, and this may be understood to be a variable that is associated with occupation and work. The results show that a higher educational level is associated with reduced prevalence of axial as well as peripheral arthrosis, and not only in load-bearing joints such as the knees, hips and lumbar spinal column, but also in the hands and cervical spinal column.
The association between the geographical area where subjects live or were born and arthrosis has always been highly interesting. In this regard the most common finding is that it is more prevalent in rural areas and less developed countries.22 However, no statistically significant differences were found in our study between those who lived in a rural or urban area. Only the incidence of lumbar spinal column arthrosis was found to be higher in rural areas, although this was not statistically significant. On the contrary, knee arthrosis showed the opposite tendency; this finding is similar to that of the EPISER2000 study, which obtained an OR of 1.74 in multivariant analysis (CI 95%: 1.09–2.77), taking “rural” category as the reference.23
Bivariant statistical analysis of the variable “having been born abroad” was associated with cervical and knee arthrosis, although neither of these associations was maintained when adjusted for age (data not shown).
Cervical spinal column arthrosis was more frequent in the Mediterranean and central areas than it was in the north, while lumbar spinal column arthrosis was more frequent in the centre. Nevertheless, knee arthrosis seems to be more common in the Mediterranean area, with an association that is close to being statistically significant.
If we compare EPISER2016 data with those of publications in other countries, the prevalence of hand arthrosis can be seen to be similar to the rate published in the Framingham cohort of the U.S.A., while the incidence of hip arthrosis is similar to the population data published in the U.S.A., Portugal, Holland and France. On the other hand, the prevalence of symptomatic knee arthrosis is higher than the figures corresponding to the U.S.A., France and Norway, and it is more similar to the figures published in Portugal, Canada and Holland (Table 6).24–26 Comparative studies of the results obtained in each country always have to be approached with caution: the selection criteria for the population as well as the diagnostic criteria used are hard to standardise, and sometimes cause results to differ or be similar in ways that cannot solely be attributed to geographical distribution. This is why, to obtain more reliable results it is desirable that populations in different countries be analysed in a single study. A good alternative would be for the next EPISER study to be undertaken in collaboration with other scientific societies in different countries, to thereby obtain figures that can be compared.
Regarding the limitations of this study, it should be pointed out that in the oldest age group (those over the age of 80 years old) the percentage of individuals who mention being in poor or very poor health in the initial questionnaire was lower than the figure in the National Health Survey of 2017 (approximately 10%–15% lower; data not shown). This may have led the prevalence of arthrosis to be partially underestimated. Moreover, in the case of knee arthrosis, although the screening NPV was high (95.12%), it was slightly below the figure for the other locations, and this may have led to a certain degree of underestimation of its prevalence.
To summarise, the EPISER2016 study is the first one to analyse the prevalence of symptomatic arthrosis in 5 locations (the cervical and lumbar spinal column, knee, hips and hands) in Spain. The study shows that the overall prevalence of arthrosis in the population ≥40 years old stands at 29.35%. It also shows that the prevalence of hand and knee arthrosis is higher than it was 16 years ago (EPISER2000), although when comparing these results, it has to be taken into account that the selected populations were of different ages, and different diagnostic criteria were used. Of all the locations studied, lumbar spinal column arthrosis is the most prevalent.
FundingEPISER2016 was financed by Celgene, Gebro Pharma, Merck Sharp and Dohme de Espana, Pfizer and Sanofi-Aventis. These financial backers did not intervene in the design of the study or data gathering and analysis, or in the writing of this paper. MS was financed by the Contrato Río Hortega-Fondo de Investigación Sanitaria (CM17/00101). The Scientific Research Fund, which is included in the National Scientific, Development and Technological Innovation Programme 2013–2016, is financed by the ISCIII-Subdirección General de Evaluación y Promoción de la Investigación- European Regional Development Fund (ERDF) “A way of making Europe”.
Conflict of interestThe authors have no conflict of interests to declare.
We would like to thank Dr. Javier Llorca Díaz for his contribution to the design of this study and Javier Prado Galbarro, for his work in the statistical analysis.
The following are the supplementary data to this article:


Please cite this article as: Blanco FJ, Silva-Díaz M, Quevedo Vila V, Seoane-Mato D, Pérez Ruiz F, Juan-Mas A, et al. Prevalencia de artrosis sintomática en España: Estudio EPISER2016. Reumatol Clin. 2021;17:461–470.


