






The objective of this study was to identify the usage and accessibility problems faced by the disabled (whether in pain or not) users of assistive devices (conventional wheelchairs), identify physical barriers that limit their mobility, and recognize the socio-cultural practices excluding them from the design process of such devices. Another main purpose of this paper is to improve the ergonomic criteria that influence the design and manufacture of assistive devices.
Materials and methodsStudy population: 15 patients with any of the following diagnoses: ankylosing spondylitis, rheumatoid arthritis, or amputees using wheelchairs in Mexico and Colombia.
DesignQualitative study. Thematic analysis with a theoretical industrial design approach for employing usability testing for ergonomic analysis.
ResultsWe identified 6 issues associated with usability problems from the patient's standpoint: barriers for use of wheelchairs (usability and acceptability), creative adaptations, potential use of technical devices, independence, body perception and assistive devices, and architectural barriers. The ergonomic and usability requirements and the resulting level of independence vary across wheelchair users with chronic pain and those whose disability does not involve pain. The latter are more independent in their movements and decisions.
ConclusionsUser input is essential in the design of assistive devices. The proposal of “design from and for the user” must rely on both engineering and medical perspective on the ergonomy as well as the user interpretation of the environment and the experience of the disease. Thus we can arrive at a “user-centered design”.
Identificar los problemas de uso y accesibilidad a los que se enfrentan las personas discapacitadas (presenten dolor o no) usuarias de ayudas técnicas (sillas de ruedas convencionales); reconocer las barreras físicas que limitan su autonomía, y registrar cuáles son las prácticas socioculturales que los excluyen del proceso de diseño de dichas ayudas.
Materiales y métodoParticiparon 15 pacientes con alguno de los siguientes diagnósticos: espondilitis anquilosante, artritis reumatoide, o amputados que utilizarán sillas de ruedas en México y Colombia. Estudio cualitativo. Análisis: temático y con aproximación teórica del diseño industrial utilizando pruebas de uso para análisis ergonómicos.
ResultadosSe identificaron 6 temas asociados a los problemas de uso desde la perspectiva del paciente: barreras que limitan el empleo de las sillas de ruedas (uso y aceptabilidad), adaptaciones creativas, independencia, potencial de uso de las ayudas técnicas (silla de ruedas y/o andaderas), percepción del cuerpo y ayudas técnicas, y barreras arquitectónicas. Las necesidades ergonómicas y de uso, así como el nivel de independencia resultante, son diferentes entre los usuarios de sillas de ruedas que sufren dolor crónico y aquellos cuya discapacidad no involucra dolor. Estos últimos tienen más independencia en sus movimientos y decisiones.
ConclusionesLa propuesta del «diseño desde y para el usuario» debe involucrar tanto las perspectivas del técnico en ergonomía y del médico como la interpretación que el usuario hace de su entorno y de la vivencia de la enfermedad.
The term “disability” refers to a physical, mental or sensory impairment, whether permanent or temporary, that limits the ability to perform one or more essential activities of daily life; this deficiency can be caused or aggravated by economic and social1,2 environments.
It is estimated that over one billion people live with disabilities. This corresponds to about 15% of the world population. In Mexico, 12% of the population has a disability, distributed as follows: 53% physical disability, 20% intellectual disability, 18% hearing impairment, and 9% visual impairment. This means that over 10 million persons in this country have some form of disability, not to mention the more than 269000 new cases that are added each year.3 An estimate for 2050 puts people with disabilities in Mexico at 22 million.4 In Colombia, in accordance with the projections of the National Department of Statistics (DANE), 12% of the population has some type of physical, sensory or cognitive disability, which is estimated at 5435394 and steadily increasing due to factors such as accidents, chronic degenerative diseases, domestic violence, and armed conflict.5 Physical disability in musculoskeletal diseases is reported to be about 13% in community studies.6 In rheumatoid arthritis (RA), specific disability is reported in 35.3% compared with 8% of the general population.7 In the case of ankylosing spondylitis (AS), functional capacity is diminished by 30 points compared to the population free of disease.8
A 2002 report of the Pan American Health Organization indicates that accessibility and mobility are the main problems facing the disabled population due to the architectural and urban barriers that intensify their difficulty integrating into the labor market and make daily9 activities difficult to achieve.
Different health problems can be crippling. Among them are those with a component of pain and inflammation, such as rheumatic diseases. We must also take into account other secondary disabilities that cause pain, such as those due to amputation or accident.
This study is based on the theoretical perspective of ergonomics and the specific needs of wheelchair use as well as the principles of user-centered design.
Ergonomics with specific needs is defined as “the discipline that allows detection of the true needs from comprehensive knowledge, understanding and working with people representing disabled users for proper projection of assistive technologies, products and spaces”.10 The potential use of wheelchairs depends not only the product but also on the user.11,12
User-centered design (UCD) proposes that designers understand the context of use of the object to be produced. This means an understanding of the environment in which daily activities are carried out by the user.10–12
Context of the StudyThe study was conducted over one year and continuously in Mexico and in Colombia. It was carried out in these two countries to perform a comparison of the changes in the adaptability of wheelchair use and disability in different social contexts. In Mexico, the study was conducted with patients without social security protection, lower class and upper class. In Colombia it was carried out with users and patients with and without social security protection, and from different socioeconomic levels.
ObjectivesThe objectives of this study are to identify the use and accessibility problems faced by disabled persons with and without pain. In addition, it seeks to identify the physical barriers that limit their autonomy and cultural practices that exclude the design process of such aids. Finally, this study seeks to enrich the ergonomic criteria that influence the design and manufacture of technical aids.
Materials and MethodsPatientsFifteen subjects were invited to participate, according to the following inclusion criteria: any gender, age 18 years or older, users of assistive devices (cane, walker and/or wheelchair), presence of pain and chronic pain and work or activities inside or outside their home. These criteria were defined in order to compare the user needs to use the same type of wheelchair, although with different disabling conditions. The same selection criteria were applied for the selection of participants in the two countries.
This study was approved by the ethics and local research committees in both countries. Informed consent letters were signed by all participants.
DesignThe present study used the qualitative research design. Qualitative research aims to explain the cultural milieu through the personal experience of the individual who serves as a theoretical and methodological basis.13–15 Qualitative methodology encompasses all designs and techniques used to collect, analyze and interpret data through narratives, documents and videos, among others. The results of qualitative research is not expressed numerically, so sample size depends on the number but not the depth and quality of information obtained in the narrative and other sources of information.16,17
Qualitative methodology has several techniques to rescue the experience of the individual, including focus groups, life histories and different forms of interviews.14–17 For this study we used the technique of in-depth interview, following a specific guide complemented by participant observation, that is, from the perspective of evaluation of ergonomics and design.
The interviews followed a guide, which was designed specifically for this study by an interdisciplinary team (social psychologist, rheumatologists, medical anthropologist, and industrial designers). Topics included in the guide were: disease context, experience of disability in the workplace and in the family, and differences in the way of life before and after the onset of disability. Additionally, we applied an evaluation of the use of assistive devices by an industrial designer (PSH). Its aim was to identify and record both the problems expressed by the interviewees as observed by the designer. This evaluation considered the biomechanics of movement, user satisfaction and performance measures of technical aids, as well as their social acceptability. The ergonomic processes ethnography was part of a practical formulation referring to an everyday situation or topic quickly identifiable, where the information obtained is qualitative, trying to bring the reality of the users of a product to the design team so that they can understand the formers’ motives, needs and demands.18 This assessment was recorded in a field journal including photographic material.
In Mexico, participants were contacted through rheumatologists working for the health sector. In Colombia, it was through a snowball17 strategy. The interviews were conducted in sessions, minimum 2 and maximum 4h per individual participant.
We studied a convenience sample that reflected the different problems of users, given its status as the basis of disability. The contact was suspended in patients who fulfilled criteria such as saturation information, that is, as the data became redundant with respect to the interview issues14 guide.
Each interview was recorded and transcribed. Both transcripts and electronic photographic records were analyzed as proposed by grounded theory analysis which consisted of the following steps:
- 1
Repeated reading of each interview, identifying issues relevant to participants using an axial coding strategy. This strategy is known as the constant comparative method based on theory.19,20
- 2
Organization of each paragraph transcribed and every fact observed (field diary and photographic record) in several categories or codes (e.g. “Independence”).
- 3
We compared the narratives to generate common themes that were closely linked and presented similarities that allowed their grouping into theme families.19
- 4
Specific semantic networks were constructed to represent the trajectory of the use of wheelchairs and/or technical assistance to each individual. This process is performed repeatedly with two reviewers with expertise in qualitative studies, looking to make a methodological triangulation when interpreting data.19,20
The analysis was conducted with the support of a qualitative analysis program, Atlas/ti v4.2. The interpretation of the data was performed based on the DCU. Topics included for interpretation were both the elements identified in the interviews and the photographic record from the theoretical proposal of specific ergonomics21 needs.
Results15 subjects participated in the study, with a mean age of 41 years. There were 6 women and 9 men. All used a wheelchair, 3 combined with a walker. Of these, eight were Mexican and 7 Colombian. The sociocultural level distribution was: 3 participants of high-income social class, 5 of middle-income class and 7 of lower-income class. There were 9 people with rheumatic diseases (4 with RA and 5 with SA). Of the 15 participants, eight of them agreed to be interviewed, photographed, and recorded. Only 2 participants agreed to the interview but not the photographic record. Of the five people in the group of users without pain who did not accept voice recordings, one of them did so on the grounds that they were in a vulnerable position and 2 did not specify the reasons.
We identified six issues concerning usability issues from the patient's perspective: barriers to wheelchairs (use and acceptability), creative adaptations, use potential, independence, body awareness and assistive technologies, and architectural barriers. These issues are detailed below and will be exemplified with excerpts from the narratives of the participants and/or photographic record.
Item 1. Barriers for a Wheelchair (Use and Acceptability)For users whose disability involves pain (patients with RA and SA), changes are observed in physical structure that directly affect bodily functions and thus, in their activities, in their accessibility to the environment and social participation. “When you walk on completely new pavement […] it is soft. But when you’re on a very bad road […] the wheelchair jumps around a lot and greatly affects my hip” (L., user Colombian, 59, RA, housewife).
When the disease is in an advanced stage, the user cannot take advantage of all the benefits it could provide due to the limitation of its movements and joint pain and swelling. “The grip is becoming increasingly difficult, the hands no longer serve me and I feel insecure sometimes, so I do not want to go out to the street” (R., user Colombian RA).
Another barrier detected which directly affects the increase of pain is due to the back and seat deformation, plastic based material that changes with use and time. “…I put a cushion on the seat so it won’t sink because My hip is at a different level and when I get in the wheelchair that I noticed increased pain in the back so I put a thinner cushion to not let me move back out. The other one produces heat”…(L., user Colombian, 59, RA, housewife).
Disabled users describe creative adaptations according to their daily needs, and they differ on whether or not the disability involves a component of pain (Fig. 1).
In the group of subjects with disabilities without pain, adaptations are related to their social needs and work: “I myself put my basket, lights and the virgin for the sale of sweets” (C., Mexican user suffering from polio, street vendor).
Unlike individuals with disabilities with pain (RA or SA), adaptations were made only at points where there was pain from the pressure of the chair: “I put a cushion for it to feel stiff and hard, so I have no vibration and does not hurt my hip” (A., RA patient, Mexican, housewife).
Using the wheelchair inside the house is usually supplemented with the walker. This is due to the inherent difficulty of maneuvering the wheelchair in a standard housing construction, which has narrow doors, stairs, etc. “[…] I feel much of a hindrance in the house with the chair, it is very large, and I cannot go to the bathroom and the wheel slips on the floor” (R., RA Mexican patient, housewife).
One of the barriers identified which directly affects the increase of pain is changes in the seat and back which are made of plastic based material and shows deformation with use and time. “…I put a cushion on the seat for it not to sink because it changes the level of my hips and when I get the wheelchair I noticed increased pain, so I put a thinner cushion on the back to not let me move back out because the other produces heat”…. (L., Colombian user, 59, RA, housewife).
Another conflict mentioned by users is the inconsistency that is generated between the wheelchair and the walker. This evidence is that walkers are simply not designed to be used in a complementary manner with a conventional wheelchair. “[…] I have to hold fast on the walker and use more force because the chair hits the walker, and is uncomfortable” (A., RA Mexican user, housewife).
Despite these limitations, there are those who feel grateful to have an element of assistance as “you can get around”: “Thank God, I have the chair; it is more harm than good but helps me sometimes here at home and almost always to go outside” (N., RA Colombian user, housewife).
Users whose disability does not involve pain have more independence in their movements and decisions. That is, while a user with a rheumatic disease need help to perform virtually all their daily activities, the amputee user has greater independence because of the potential they have to get used to their new circumstances (Fig. 2). “Sometimes I am very sorry for my family, to be asking for the favor, to be helping me for everything […] I do not go out much because I need to ask others for help […] I do not like to disturb” (F., SA Mexican User).

These descriptions are more frequent in the group of users with more pain and disability. They are less common among those patients who highlight the dearth of outdoor activities due to pain and also have a low tolerance for assistive device, and who also often feel like “a burden” to their families. “After that I felt bad because I could not work […] and hardly do anything […] I cannot help around the house” (L., RA Colombian user, housewife).
There are 2 types of narratives about the perception of the body and aids.
They are those who perceive their body “integrated” to the aid (generally those whose disability lacks pain) and, therefore, do not identify major constraints for movement and independence. “[…] It's my working tool, in addition, I can cross the street and I sprint with my arms” (C., Mexican user, disabled painless peddler).
Furthermore, in the chronic pain group, members refer to technical aids as foreign to their body. In general, the perception of embedded aids in society is negative. “[…] Because I felt that I looked weird and I felt embarrassed, sad, depressed […]I saw myself in that situation, limited state, I could not walk” (F., Mexican RA user).
Architectural barriers described and identified in the assessment of potential use were found in the home, the workplace and/or outdoors, so users live with a constant sense of limitation. Outdoors, the clear barrier is the lack of application of design standards for persons with disabilities, such as ramps, parking spaces and ample space for movement. “…Here at home I can only move in the room, with the chair I cannot go to the bathroom because it is not by the door into the kitchen, it is impossible, and in the streets, almost no ramps. The platforms are very high and my husband cannot help me because he is not strong enough” (N., RA Colombian user).
The 2 groups with disabilities (with pain, no pain) described narratives of barriers faced by users of assistive devices (wheelchairs and/or walkers), and also point to the existence of social barriers. Usage problems were identified in both the disability group with pain (RA/SA) and those without. Example of these problems are related to the fact that standard wheelchairs do not meet the requirements of safety and comfort that users require to meet their needs.
The main difference between the two groups was that, due to the inconsistency with this technical issue, people who have no pain adapted chairs trying to improve their potential for use and tried to give identity, thus making it part of their body. By contrast, people who have pain only made minor adjustments, such as using pillows to raise the seat height, and generally tried to use the chair as little as possible at home, given the multiple barriers they encountered. These patients also expressed disagreement with the feeling when using aids, considering themselves ‘distressed’. Until recently, the objects used by the disabled were manufactured by the specialized medical equipment industries, providing them with a character that could be considered formal, cold and unpleasant, especially from the perspective of people who, despite their deficiency are not considered sick. An ergonomically correct approach to the design should incorporate the specific requirements of these populations, resulting in compatible solutions with any user.21
Importantly, first, we discarded fundamental aspects that could be the user's own barriers, such as lack of good posture. To test this possibility, we found that the seat and back are simply not suitable for a good back posture, favoring deviations. Furthermore, it was shown that a correct position of the pelvis is difficult to obtain because it slid on numerous occasions. To avoid this it would take height-adjustable footrests and a good restraint system. Consequently, people with disabilities cannot comfortably use conventional aids, unless they have been modified with attachments designed by the user. All the evidence from this study suggests that the aid is not designed to allow users to meet their needs. This can lead to situations of abandonment or underutilization of aids, with the consequent negative impact on the quality of life of users.
The design and use of unsuitable wheelchairs lead to the need to increase family protection and care for the disabled person. As a result, there is a loss of independence, expressed by the participants in this study. This creates constant feelings of insecurity and functional dependence, which leads to low social22 acceptability.
We also observed that users whose disability involves pain begin to experience problems of wheelchair accessibility and acceptance problems. In this they differ from those free from chronic pain, as the latter seek to form an identity with the wheelchair to optimize their use in everyday life, such as adding attachments themselves (mirrors, lights, etc.). However, where both groups find their greatest barrier is in the urban environment. Technical assistance should be intended to allow the user maximum functionality, comfort, and mobility. To meet this goal, the seat, for example, must be designed to fit the person.23 That is, the goal is simply to serve for movement, regardless of the technical assistance aspects considered as an intermediary to facilitate the integration of the disabled person to society.24
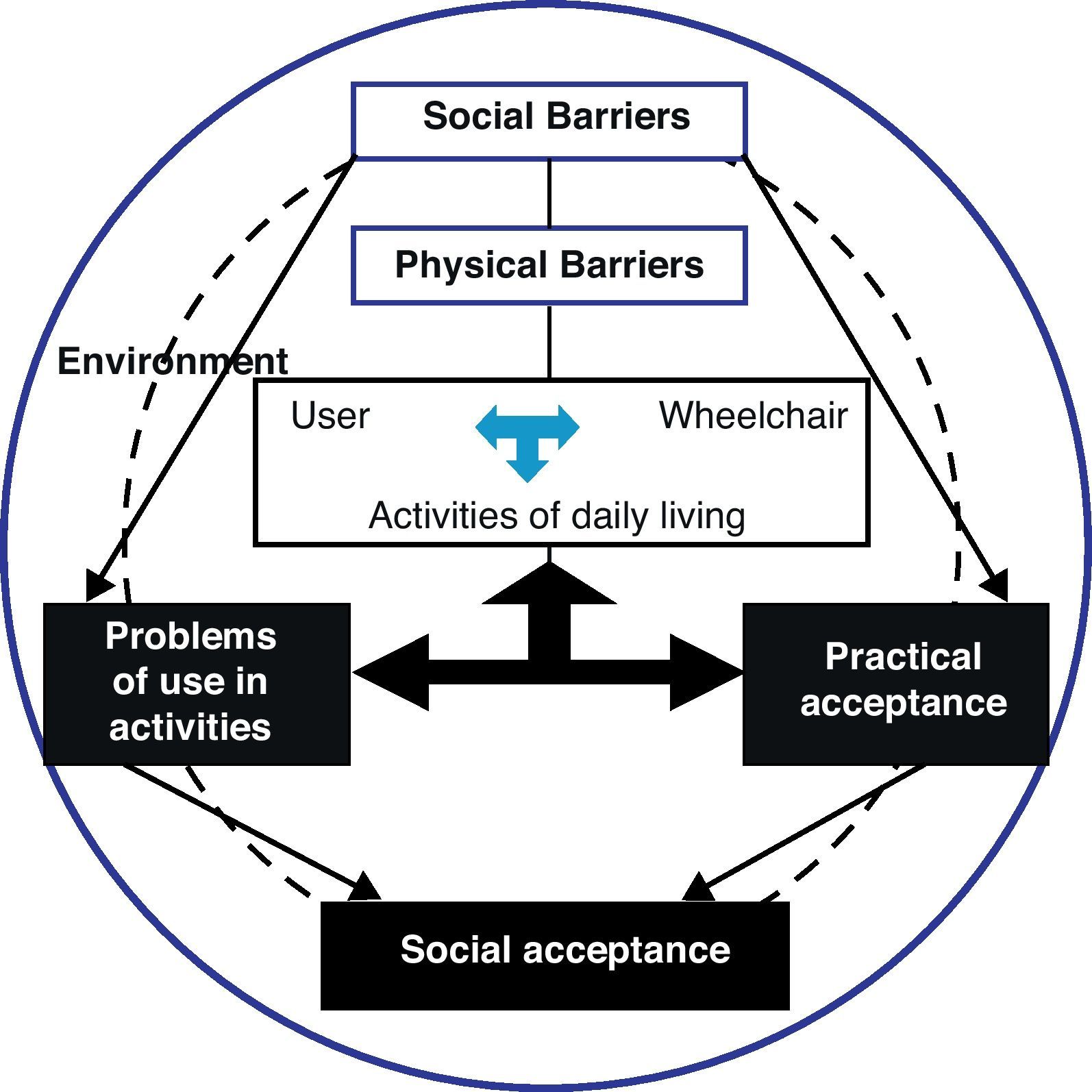
The problems of using an aid are directly related to their acceptance. This affects the social approval that the user perceives in their social environments, due to physiological and functional aspects involving their disease (Fig. 3).

Therefore, the designer must be able to act as a link25 between “possible” (what the technique available to us offers) and “desirable” (what society, or part of it, might want).26,27
The user-centered design, a universal design (The Center for Universal Design, 1997), social integration and potential access are issues that emphasize security requirements and the elimination of architectural and urban barriers.27,28
Limitations of the StudyThe findings of this study are limited in their application because they are only useful in the context of developing societies that do not have adequate architectural infrastructure for people with disabilities, or where there are restrictions on the purchase of electric wheelchairs.
ConclusionsBoth subjects with pain and disability in patients with rheumatic diseases, as well as those without pain, manifested both the need to use assistive devices (wheelchairs and/or walkers), as well as specific architectural requirements. These needs and requirements are different between the 2 groups.
The contributions and user views are critical to the success of a design, both from the designer and the user. We propose the integration of perspectives and medical technicians with the experiences of people with disabilities, the latter being the direct users of mechanical support.
Conflict of InterestThe authors have no conflict of interest to declare.
We thank Dr. Leticia Lino Perez for providing the facilities for conducting the fieldwork for this project.
Please, cite this article as: Herrera-Saray P, et al. Problemas con el uso de sillas de ruedas y otras ayudas técnicas y barreras sociales a las que se enfrentan las personas que las utilizan. Estudio cualitativo desde la perspectiva de la ergonomía en personas discapacitadas por enfermedades reumáticas y otras condiciones. Reumatol Clin. 2013;9:24–30.


