






Osteoarthritis (OA) is considered the most common degenerative joint pathology in the adult population, being an important cause of disability worldwide, and its prevalence is increasingly associated with different factors, including obesity. Obesity together with metabolic syndrome have been associated with a pro-inflammatory state due to the release of cytokines that induce changes in cartilage metabolism. Chemerin is an adipokine secreted mainly by adipocytes and its final action is to increase the production of IL-6, IL-8, IL-1b, TNF-a and metalloproteinases by macrophages, dendritic cells and chondrocytes, which are responsible for damage to the articular cartilage. This is one of the reasons that obesity and inflammation have been linked to OA. The main objective of this study is to determine whether the serum chemerin concentrations of a group of patients with primary OA are higher when compared with control individuals. A further purpose of the study is to determine the relationship between the presence of obesity/overweight with the severity of the disease measured by a radiological scale.
Patients and methodsAn analytical cross-sectional study was carried out where serum chemerin levels were quantified by enzyme-linked immunoadsorption assay (ELISA), in patients with primary OA of the hip, knee and hand with criteria from the ACR (American College Of Rheumatology) and controls. Radiological studies of patients and controls were analysed to determine the severity of joint involvement using the Kellgren and Lawrence (KL) classification system. The statistical significance of the difference in serum chemerin values between the two groups was verified and the correlation between the variables of body mass index (BMI) with radiological severity, number of joint regions and serum chemerin levels was analysed.
ResultsDuring the period from July 2015 to July 2016, serum samples and radiographs of compromised joints were collected from 40 patients with primary OA who met the inclusion criteria, as well as serum samples from 20 controls. The average concentration of chemerin was higher in the group of patients with OA compared to that of the control group, being 373ng / ml and 175.55ng / ml respectively (p<2.2×10–16). No significant associations were found between the different degrees of disease severity measured by the KL radiological scale, such as the number of involved joint regions and BMI.
ConclusionsIn a group of patients with primary OA of the hand, knee or hip, the values of chemerin were higher than those found in controls, without significant association with the severity of the disease established radiologically by K/L scale, the number of involved joint regions, and the BMI.
La osteoartritis (OA) es considerada como la patología articular degenerativa más frecuente en la población adulta, siendo una causa importante de discapacidad a nivel mundial y su prevalencia va en aumento asociada a diferentes factores entre ellos la obesidad.
La obesidad junto con el síndrome metabólico se han asociado con un estado pro inflamatorio debido a la liberación de citocinas que inducen cambios en el metabolismo del cartilago. La quemerina es una adipocina secretada principalmente por adipocitos y tiene como acción final, el aumento de la producción de IL-6, IL-8, IL-1b, TNF-a y metaloproteinasas por parte de macrófagos, células dendríticas y condrocitos, las cuales son encargadas del daño del cartílago articular. Esta es una de las razones por la que se ha relacionado la obesidad y la inflamación con la OA. El objetivo principal de este estudio consiste en determinar si las concentraciones de quemerina en suero de un grupo de pacientes con OA primaria son mayores al compararlos con individuos controles sanos; y adicionalmente determinar la relación entre la presencia de obesidad/sobrepeso con la severidad de la enfermedad medida por una escala radiológica.
Pacientes y métodosSe realizó un estudio de corte transversal analítico donde se cuantificaron los niveles de quemerina en suero mediante ensayo por inmunoadsorción ligado a enzimas (ELISA), en pacientes con OA primaria de cadera, rodilla y mano con criterios del ACR (American College Of Reumathology) y controles sanos. Se analizaron los estudios radiológicos de los pacientes y controles para determinar la severidad del compromiso articular aplicando el sistema de clasificación de Kellgren y Lawrence (KL). Se verificó la significancia estadística de la diferencia de los valores de quemerina sérica entre los dos grupos y se analizó la correlación entre las variables de índice de masa corporal (IMC) con severidad radiológica, número de regiones articulares y niveles de quemerina sérica.
ResultadosDurante el período de julio de 2015 a julio de 2016 fueron recolectadas muestras de suero y radiografías de las articulaciones comprometidas de 40 pacientes con OA primaria que cumplieron los criterios de inclusión, así como muestras de suero de 20 controles sanos. La concentración promedio de quemerina fue mas alta en el grupo de pacientes con OA comparado con el con el grupo control, siendo de 373ng/mL y 175,55ng/mL respectivamente (p<2.2×10-16). No se encontraron asociaciones significativas entre los diferentes grados severidad de la enfermedad medida por escala radiológica KL como con el número de regiones articulares comprometidas y el IMC.
ConclusionesEn un grupo de pacientes con OA primaria de mano, rodilla o cadera, los valores de quemerina fueron superiores a los encontrados en los controles sanos, sin asociación significativa con la severidad de la enfermedad establecida radiológicamente por escala K/L, el número de regiones articulares comprometidas y el IMC.
Osteoarthritis (OA) is a multifactorial degenerative joint disease characterised by deterioration of the joint cartilage, changes in the subchondral bone, formation of osteophytes and synovial inflammation.1 It is considered the most common joint disease2 and is one of the main causes of disability in the USA, with more than 22.7 million people reported to have activity limitations.3 The estimated prevalence and incidence vary according to the definition of OA, the specific joint, and the study population.4
An article reported in Colombia evaluated 6693 people from 6 cities and established OA as the most prevalent rheumatic disease (10.81%; 95% CI: 9.68%-12.06%), data close to those found worldwide.5 OA has been associated with reduced quality of life. In 2003 it was estimated as the sixth cause of disability worldwide, and is expected to be the fourth cause by 2020.6
It has been estimated that the prevalence of OA will increase due to several concomitant factors such as population growth and aging due to increased life expectancy, increased overweight and the prevalence of obesity. Furthermore, it has been considered that OA may lead to an increase in cardiovascular morbidity due to decreased physical activity.3 Among the risk factors associated with the development of OA, age is the most strongly associated risk factor, due to the physiological changes in cartilage that occur with ageing,2 followed by obesity and metabolic disease, and it is considered an inflammatory and biomechanical disorder.7
There is growing interest in research into adipokines because although obesity and overweight are risk factors for the development of OA and attributed as mechanical components, there are studies that support metabolic factors that contribute to development of the disease.8 Adipose tissue is currently considered an endocrine organ that is metabolically active, secreting pro-inflammatory cytokines and adipokines that have been linked to the pathophysiogenesis of OA (leptin, resistance, adiponectin).8,9
A new adipokine called chemerin, secreted by adipocytes, endothelial cells, synoviocytes and chondrocytes, has recently been investigated and may establish a relationship between obesity, BMI, joint inflammation and cartilage degradation,10 independent of the mechanical factor considered to be the cause of joint involvement. Not only does chemerin have a metabolic function, but it has recently been shown to have potent chemotherapeutic activity through the chemerin receptor 23 (Chem23) with increased expression of TNF, IL1-β, IL-6, MMP-1, and MMP-8 in human joint chondrocytes.11 High chemerin titres induce MMP-2, MMP-3, MMP-13 and IL8, which have been linked to degradation of joint cartilage.12 Studies of chemerin levels in patients with OA are scarce and have diverse results. Increased chemerin levels have been found in patients with knee OA related to levels of C-reactive protein, IL-6, and IL-6 and TNF-α13,14 suggesting an inflammatory component. Valcamonica et al.13 report contradictory results showing that they found no significant difference in serum chemerin levels performed in 11 patients with OA, 8 patients with psoriatic arthritis and 18 patients with rheumatoid arthritis. These results contrast with the results of studies conducted by Ma et al.15 where chemerin levels were higher at the synovial fluid and membrane level in patients with knee OA compared to healthy subjects. Hung et al.12 also report increased levels of serum chemerin and synovial fluid in patients with knee OA.
Other studies have evaluated the relationship between serum chemerin levels and the radiographic severity of OA. In this regard Duan et al.14 report the association of increased serum chemerin levels with increased radiological involvement and increased BMI in patients with knee involvement.
The main objective of our study was to determine whether serum chemerin concentrations in a group of patients with primary OA in the hand, knee and hip are higher when compared to healthy controls, and to determine the relationship between the presence of obesity/overweight with severity of disease as measured by a radiological scale.
Patients and methodsA cross-sectional, analytical study was conducted in Colombian patients over the age of 18 from July 2015 to July 2016. Forty patients with a diagnosis of primary OA of the hand, knee and hip were recruited according to the criteria of the American College of Rheumatology (ACR),16,17 and 20 healthy individuals as controls. Serum samples were collected, and X-rays of the affected joints were taken from both patients and controls following identical protocols. The inclusion criteria for OA patients included 1) a score ≥2 on the Kellgren and Lawrence (K/L) radiological severity scale18 and 2) authorization of participation by signing informed consent. The healthy controls were selected from the outpatient clinics of other medical services, with the following inclusion criteria: a) individuals over 18 years of age without clinical evidence of primary or secondary OA by means of a clinical questionnaire and physical examination by the rheumatology department, and b) willingness to participate in the study after authorisation by signing informed consent. The exclusion criteria for the 2 groups studied were a) patients with secondary OA (history of surgery, trauma or injury to the ligament in the joint to be assessed); b) patients with active infectious disease; c) patients diagnosed with rheumatoid arthritis, systemic lupus erythematosus, reactive arthritis, seronegative spondyloarthropathy, arthropathy due to crystal deposition (monosodium urate, hydroxyapatite, calcium pyrophosphate); d) clinical symptoms suggesting any other chronic inflammatory condition in the judgement of the treating physician; and e) history of corticoid use in the last 3 months.
Anteroposterior hand, knee and hip x-rays were taken 6 months before the serum sample was taken and were analysed by 2 doctors trained in the KL grading system: grade 0, no radiological changes; grade 1, doubtful change in joint space narrowing and possible osteophyte formations; grade 2, defined osteophytes and possible joint space narrowing; grade 3, moderate multiple osteophytes, definitive joint space narrowing, sclerosis and possible deformity of the bone contours; grade 4, large osteophytes, marked joint space narrowing, severe sclerosis and defined deformity of the bone contours. Weight and height measurements were made with a calibrated instrument for calculating body mass index (BMI), according to the formula BMI=weight in kg divided by height in cm2. BMI≥25 was considered obesity or overweight. This index was not considered in the selection of patients, to prevent selection bias in the final analysis.
The time of disease onset was defined as when the patient became aware of symptoms such as stiffness, mild to severe inflammation of the involved joint, pain on joint movement, or use of hip, knee, or hand orthoses for longer than 3 weeks in the last 6 months prior to the start of the study.
Serum samples were taken from the 40 patients with primary OA and the 20 healthy controls. Chemerin levels were quantified by capture ELISA (ab155430 ABCAM Chemerin Human ELISA KIT) in duplicate, using a biotinylated anti-human antibody and a conjugate (Streptavidin-HRP). The values obtained were evaluated against a standard curve provided by the kit, using recombinant human chemerin. Reading of the test was at 450nm by spectrophotometry. The sensitivity of the test is .5ng/mL.
For the statistical analysis, a general descriptive analysis of the demographic variables was undertaken to characterize the patients involved in the study. Patients were classified using different criteria such as age, gender, body mass index, joint(s) affected and K/L levels. Differences in mean chemerin levels between groups of patients with OA were explored and chemerin levels between patients with OA and control individuals were compared. Median polish (Hoaglin et al. 1983) was used for two-way analysis between different K/L grades (grade 0, grade 1, grade 2, grade 3 and grade 4). Student’s t-tests for mean differences were applied with the Welch modification for degrees of freedom, and the mean chemerin level of each group was determined by estimating confidence intervals. Inference is made at a 95% confidence level. R 2017 (The R Project for Statistical Computing) was used.
The study protocol was approved by the ethics committee of the National University of Colombia and the committees of the hospitals where the patients were recruited. All participants provided written informed consent. The study meets the requirements for human research according to resolution 8430 of 1993 of the Ministry of Health of the Republic of Colombia and in accordance with the ethical norms and standards in human research of the Declaration of Helsinki of 1964.
ResultsSerum and X-ray samples were obtained over the period July 2015 to July 2016, from 40 OA patients and 20 healthy controls. In relation to the demographic characteristics of the groups, there were more females (92%) in the OA group than in the control group (55%). The average age was 64.8 and 65.7 of patients and controls, respectively, and the BMI was higher (26.59) in the OA group compared to the control group. The average disease duration for patients with OA was 6.9 years (Table 1).
Characteristics of patients with OA and of the control group.
| Patients with OA (n=40) | Control group (n=20) | |
|---|---|---|
| Age in years; mean | 64.8 | 65.7 |
| Time of onset in years; mean | 6.9 | — |
| BMI; mean | 26.59 | 25 |
| Female; % | 92% (37) | 55% (10) |
| Likelihood ratio; genders | 11.68344; p=.0001653 | |
| 95% CI: 2.428822;78,705047 |
BMI: Body Mass Index; OA: Osteoarthritis.
Description of patients and controls: mean values of age, time of onset and BMI. A predominance of females can be observed in both groups. The Student’s t-test for difference in means and the Welch test for calculating degrees of freedom are used.
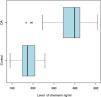
Chemerin values were higher in the OA group (373.525ng/mL) compared to the control group (175.55ng/mL), with a p<2.2×10−16 (Table 2, Fig. 1). Meanwhile, no significant associations were found in relation to BMI or age when comparing the 2 groups (Table 2).
Comparison of chemerin levels, age and BMI between controls and patients with OA.
| Control | OA | t | p value | 95% CI (control OA) | |
|---|---|---|---|---|---|
| Chemerin; ng/mL | 175.55 | 373.525 | −11.586 | 2.2×10−16 | (−232.213;−163.737) |
| Age | 66.05 | 64.375 | .666 | .509 | (−3.378;6.728) |
| BMI | 25.23 | 26.509 | −1.768 | .083 | (−2.729;.171) |
BMI: Body Mass Index; OA: Osteoarthritis; t: Student’s t-test.
No statistical differences are observed when comparing mean chemerin levels with respect to BMI or age. Note the significant differences between the chemerin levels of the patients with OA compared with the control group (2.2×10–16). The Student’s t-test for difference in means and the Welch test for calculating degrees of freedom are used.
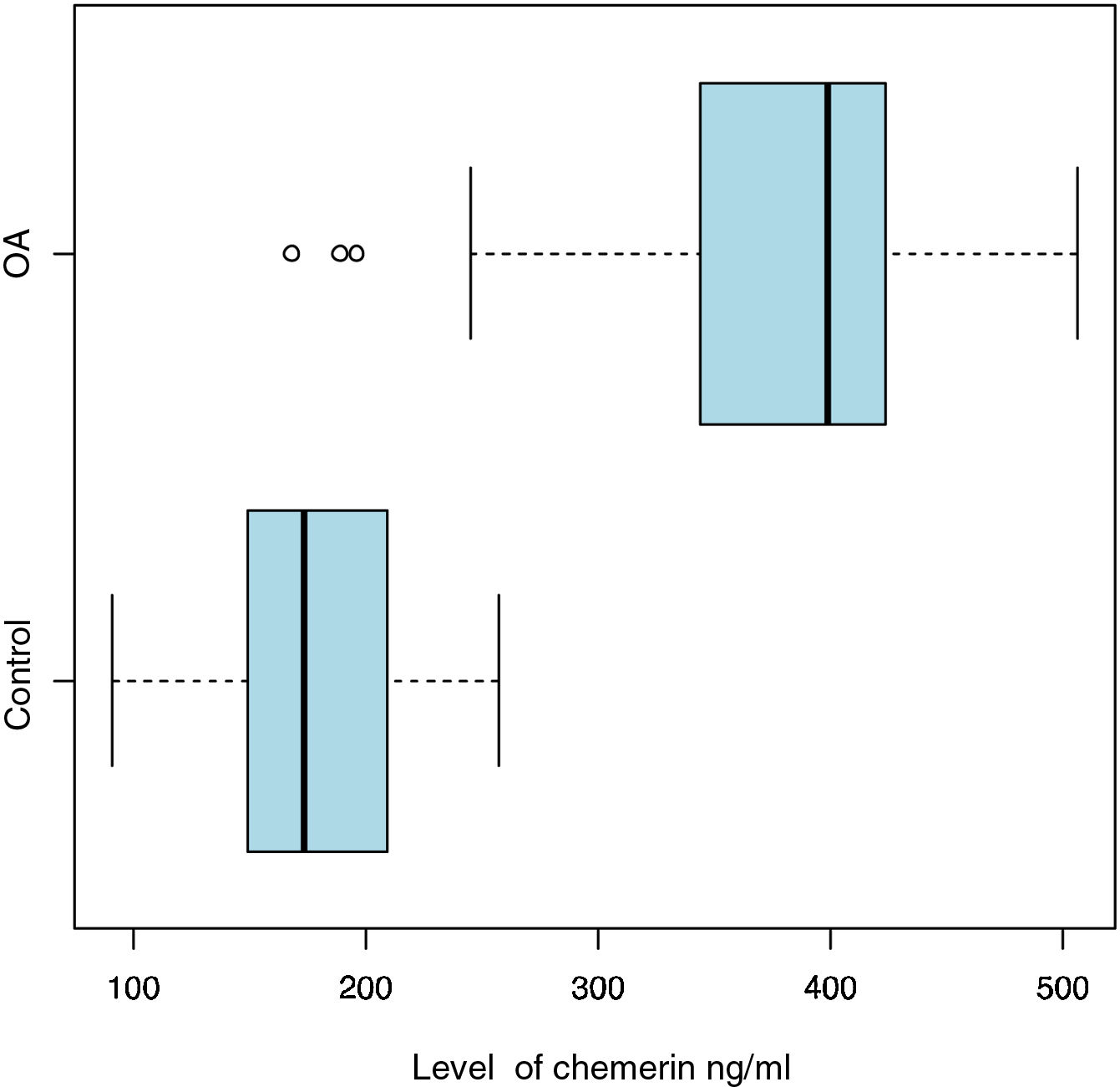
Chemerin levels in patients with OA and controls. At a 95% significance level (163,737 and 232,213), the difference between average chemerin levels of patients with OA and the control group is statistically significant (p<2.2×10−16). The Student’s t-test for difference in means and the Welch test for calculating degrees of freedom are used.
Regarding the clinical characteristics in the group of patients with primary OA, 65% showed involvement of a joint region, of which there was involvement in the hand in 47.5%, in the knee in 7.5%, and in the hip in 10%. The remaining 35% of patients had involvement of more than one different joint at the time of the study, where 25% had involvement of 2 joint regions and 10% had involvement of 3 joint regions. Table 3 shows the percentage of chemerin levels in patients with OA in each group and the different combinations of joint involvement, from one to three involved joints. Among the groups studied the highest percentage of chemerin levels was found in the patients with hip OA (95% CI: 189.8819 and 278.3286).
Clinical characteristics of OA patients. Joint regions involved and chemerin levels compared to the healthy control group.
| Osteoarthritis | OA | t | p value | 95% CI (control OA) | N | Percentage |
|---|---|---|---|---|---|---|
| Only one joint affected | 364.8621 | −8.9812 | 1.383×10−11 | (−230.1237;−145.8110) | 26 | 65 |
| Only 2 joints affected | 409.5000 | −14.3940 | 1.523×10−13 | (−265.9012;−199.3093) | 10 | 25 |
| All 3 joints affected | 400.0000 | −13.0210 | 2.532×10−7 | (−261.6219;−184.5887) | 4 | 10 |
| Only the knee | 348.0000 | −5.4889 | .0155 | (−276.72289;−65.48764) | 3 | 7.5 |
| Only the hand | 345.1579 | −6.2559 | 1.276×10−6 | (−223.5499;−112.9764) | 19 | 47.5 |
| Only the hip | 411.0000 | −12.3740 | 3.196×10−6 | (−278.3286;−189.8819) | 4 | 10 |
| Only the knee and hand | 407.7500 | −16.4340 | 5.177×10−12 | (−260.4479;−201.2626) | 4 | 10 |
| Only the knee and hip | 402.3333 | −12.7720 | 1.434×10−5 | (−268.6475;−182.2297) | 3 | 7.5 |
| Only the hip and hand | 419.0000 | −6.0032 | .01727 | (−391.41361;−92.79691) | 3 | 7.5 |
95% CI: 95% Confidence Interval; OA: Osteoarthritis; t: Student’s t-test.
Note the percentage of patients with involvement of one or more joints. At a 95% confidence level, in all cases the patients’ chemerin levels are significantly higher compared to the controls. However, of those with involvement of only one joint the highest levels are found in those with hip involvement (95% CI 189.8819 and 278.3286). The control group’s chemerin levels were 175.55ng/mL.
Finally, when evaluating chemerin levels with the degree of radiological involvement using the K/L method in each of the groups of patients with OA, a significant relationship was found by analysis of variance (p<.00172) in patients with hand involvement associated with a higher radiological degree (K/L4>K/L3). However, no significant associations were found with the other involved joints and the degree of radiological severity with each group of patients.
DiscussionOA has long been considered a degenerative disease of the joint cartilage. This paradigm has changed in recent decades and it is now considered an inflammatory disease that involves the entire joint apparatus and ends in progressive damage to the hyaline cartilage, subchondral bone, formation of osteophytes, and limitation of joint function accompanied by severe physical disability.
It is also the most common joint disease present in adults and the cause of most disability worldwide. In Colombia we have no data on prevalence, the frequency of its clinical phenotypes and the physical disability it generates, or on the economic impact on the health system.
Our results show that OA was more frequent in females (92.5%) with an average age of 64.88 (32–79) years, and average disease progression of 6.9 years. We know that this depends on specific variables for each population under study such as its increase with age, genetic factors, socio-cultural and occupational factors that directly influence early onset or delay of symptoms. Our results are within the general characteristics reported for the disease in the literature.
We were struck by the fact that, involvement of the hand (involving some PIP, DIP and CMC joints) was present in 47.5% of the patients in our study, involvement of the hip in 10%, and of the knee in 7.5% (Table 3). These clinical presentation data of OA are important since in Colombia and Latin America we do not have studies that provide this information. Most studies establish knee OA as the most frequent form of clinical presentation.6 Our results also contrast with the study by Hunter et al.,19 which showed hand involvement to be present in 6% of adults around 30 years of age and 13% of adults over 60 years of age. We did not find hand involvement in young adults perhaps because there was no selection bias in this regard in the inclusion of our patients. Other studies of OA in ethnic populations like ours, such as in the Mexican population, report the prevalence of primary OA as 10.5% (95% CI: -10.1–10.9) being more frequent in females (11.7%) and males (8.7%). Involvement of the hand was also relevant in 43.3%, and of the knee and hip 23.9% and 10.9%, respectively.20 Recently, chemerin21 has been identified as a new adipokine that regulates the development and functioning of the adipocyte and the glycosidic metabolism in the liver and the skeletal muscle in the same way. Several investigations have linked high levels of chemerin in the blood to obesity and some aspects of metabolic syndrome. Thus, it has been investigated how this cytosine secreted by adipocytes, endothelial cells, synoviocytes and chondrocytes can establish a relationship between obesity, BMI, joint inflammation, and cartilage degradation10 independent of the mechanical factor considered to be the cause of joint involvement. Clinical studies linking chemerin levels to OA are scarce and there is considerable heterogeneity in their results. Increased levels of chemerin have been found in patients with knee OA related to levels of C-reactive protein, IL-6 and TNF-α13,14 suggesting a relationship with the inflammatory component in OA. However, some other clinical studies in this regard have shown heterogeneity in their results.12–15 Huang et al.12 found significant association in patients with knee OA and serum and synovial fluid chemerin levels related to a higher degree of joint severity of the disease. Similarly, Ma et al.15 found increased serum chemerin in patients with knee OA in synovial fluid and membrane compared to healthy subjects, establishing the possible relationship of this cytokine in the pathogenesis of OA. These studies contrast with the work carried out by Valcamonica et al.13 where they compared levels of serum chemerin without finding significant associations in a total of 37 patients, of which 18 had rheumatoid arthritis, 8 psoriatic arthritis and 11 OA. Other studies, such as that by Bozaoglu et al.,22 relate serum chemerin levels to components of metabolic syndrome such as triglyceridaemia, blood pressure, insulin resistance and body fat. They even set a plasma chemerin concentration of 240ng/mL as the cut-off point for establishing the association with metabolic syndrome with a sensitivity of 75% and a specificity of 67%. This result is valuable in the sense that there are no reports on cut-off points of plasma chemerin levels related to joint disease. We found levels of 373,525ng/mL as the average value in patients with OA, with a significant association (p<2.2×10–16) compared to healthy controls where the average value was 17,555ng/mL (Table 2 and Fig. 1). Our purpose in this study was also to know the relationship between patients with OA, obesity, and serum chemerin levels. Most of our patients compared to controls, were in the overweight range with average BMI levels (26,509) and (2523), respectively. We found no patients in the obesity range. These data agree with the reports of previous studies mentioned above that imply that these high levels of chemerin may be participating in the aetiopathogenesis of OA, and that, despite its secretion by adipose tissue, it is elevated in OA even if there is no obesity, due to the characteristics of the population studied. For this reason, it is highly likely that no significant association has been found between ranges of chemerin and obesity levels as shown in Table 1. Also, within the objectives we sought to assess in this study was the relationship between the levels of serum chemerin, BMI and radiological severity and the different clinical phenotypes found in our patients. The information found in the different studies on this aspect is also contradictory.13,14 We found no correlation between chemerin levels with the number of joint regions involved and the severity of disease measured by the K/L radiological scale, nor its relationship with BMI, unlike the data reported by Duan et al.14 who found a significant association between these variables specifically in knee OA. Nevertheless, and in accordance with the above, it is important to mention that we observed a higher secretion of chemerin in the patients with OA of the hand classified as KL/4 compared to KL/3 with a statistically significant association (p<.00172).
Most previous studies have evaluated chemerin values only in relation to knee OA with increased BMI12,14 however, in our study we included patients with OA with hand, hip and knee involvement, thus avoiding the biomechanical factor associated with obesity which could cause confusion when evaluating chemerin levels. We would like to highlight that this is the first study in a Colombian and Latin American patient population that includes patients with primary OA, and that cross-sectionally evaluates levels of serum chemerin and its possible association with the disease with certain clinical associations such as BMI and disease severity measured by a radiological scale. Similarly, it is interesting to note that OA is not only due to mechanical factors, but metabolic factors are also involved in the pathogenesis of the disease, as has been sufficiently demonstrated in OA of knee, hip, and hand joints. We are aware of the limitations of this study which include the low number of patients, which could affect the detection of some other epidemiological variables with significant differences between patients and controls. As this is a cross-sectional study design, only associations can be established, not a causal relationship. What it does allow us to do, in general terms, is to observe the behaviour of OA in our setting with other patient cohorts in other latitudes.
The most important finding of our research study was that serum chemerin levels were slightly more than double in patients with OA (373,525ng/mL) compared to healthy controls with a significant association of (p<2.2×10–16) (Table 2 and Fig. 1), but without a significant association with clinical phenotypes, which is attributed to the size of the study sample. According to our findings, in the future we will be able to conduct studies with a greater and more varied number of patients considering additional clinical variables, related to metabolic syndrome and other clinical aspects related to the pathophysiology of the disease, including the involvement of various joint regions.
ConclusionsWe can conclude in this study, that in a group of Colombian patients with primary OA with hip, knee, and hand involvement, chemerin values are higher than in healthy controls without a significant association with the degree of disease severity established by the K/L radiological scale, BMI, number of joint regions involved and clinical phenotype.
FundingFunding entities: National University of Colombia. Hermes code: 28088. Colombian Association of Rheumatology. Acta 9 award. Best research work 2016.
Conflict of interestsThe authors have no conflict of interest to declare.
We would like to thank the Hospital Simón Bolívar and the Clínica Fray Bartolomé de las Casas for allowing the research, and the Colombian Association of Rheumatology for funding the project.
Please cite this article as: Cajas Santana LJ, Rondón Herrera F, Rojas AP, Martínez Lozano DJ, Prieto N, Bohorquez Castañeda M. Quemerina sérica en una cohorte de pacientes colombianos con osteoartritis primaria. Reumatol Clin. 2021;17:530–535.


