





Pyomyositis, an acute bacterial infection of skeletal muscle, is caused by Staphylococcus aureus or other gram-positive organisms in >90% of cases. A 19-year-old boy with severe idiopathic aplastic anemia presented a pyomyositis of inner thigh muscles due to Escherichia coli as a complication of his underlying disease. The diagnosis was established by means of soft tissue ultrasound, magnetic resonance imaging (MRI) and blood culture. Surgical debridement and antibiotic treatment were performed. Postoperative course was uneventful and pyomyositis was successfully resolved. Pyomyositis caused by E. coli is uncommon condition, and very few cases have been reported, most of them being severe immunodeficiency patients, but we should know the existence of this entity and its management.
La piomiositis es una infección bacteriana aguda del músculo esquelético que es causada por Staphylococcus aureus u otros organismos gram positivos en >90% de los casos. Presentamos el caso de un hombre de 19 años de edad con anemia aplásica idiopática severa quien presentó una piomiositis de los músculos internos del muslo debido a Escherichia coli como una complicación de su enfermedad de base. El diagnóstico se estableció por medio de ultrasonidos de tejido blando, resonancia magnética (RM) y hemocultivo. Se llevaron a cabo desbridamiento quirúrgico y tratamiento antibiótico. El postoperatorio transcurrió sin complicaciones y la piomiositis se resolvió con éxito. La piomiositis causada por E. coli es una condición poco común, y muy pocos casos han sido reportados, la mayoría de ellos son pacientes con inmunodeficiencia grave, pero debemos conocer la existencia de esta entidad y su tratamiento.
Pyomyositis is an acute bacterial infection of skeletal muscle that can affect the general population in tropical climates or immunocompromised patients in general. Although it can occur at any age, it is more common in tropical climates affecting children 5–9 years and young adults, and in temperate climates, adults between 20 and 40 years. By gender ratio is 2–3/1 in favor of males. Its incidence is increasing in Western countries, especially in patients with chronic debilitating diseases such as diabetes mellitus, hematological diseases, connective and HIV infection. Staphylococcus aureus or other gram-positive organisms are the causative agents in more than 90% of cases. Pyomyositis due to Escherichia coli is an unusual condition.1,2
Pyomyositis usually begins with a very subtle clinical presentation thus being difficult to diagnose in early stages. The initial symptoms are diffuse crampy pain and tenderness on the involved area, usually followed by edema, low-grade fever and leukocytosis depending on the underlying disease the patient may have.2 Nowadays, MRI is the most reliable study to make a diagnosis of pyomyositis.3 First-line treatment consists of draining the abscess, if any, by surgery or percutaneous puncture guided by ultrasound or CT and intravenous antibiotic treatment.4 Herein we present a case of pyomyositis induced by E. coli.
Clinical observationA 19 year-old boy with severe idiopathic aplastic anemia diagnosed when he was 7 (with history of bleeding and pulmonary infection, treated with transfusions and antibiotics respectively, and outstanding bone marrow transplant) was admitted to the pediatric department after he came to the emergency department of our hospital presenting fever and a painful, erithematous and indurated skin area located on the inner left thigh, of 48h of evolution. The blood exam showed 200×109/l leukocytes and C-reactive protein of 390mg/dL and axillary temperature was 37.5°C.
Empirical treatment with iv cefepime (6g/d) and iv amikacin (15mg/kg/d) was immediately started being changed four days later after blood cultures were positive for E. coli. According to the antibiogram, treatment was changed to cefuroxime (4.5g/d) and amikacin (15mg/kg/d) during three weeks.
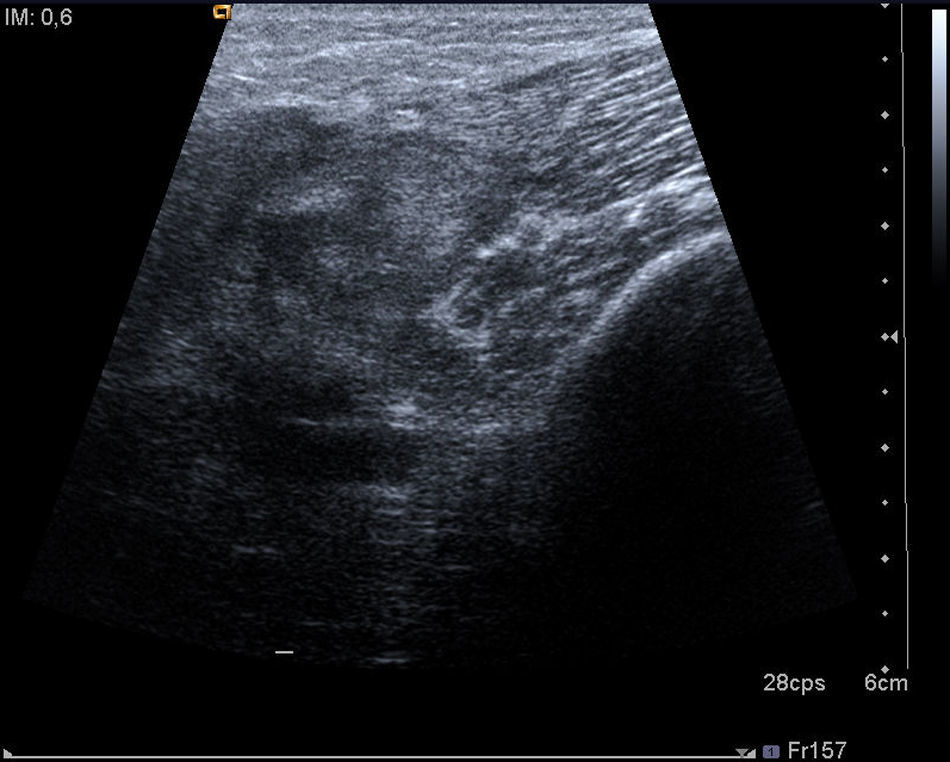
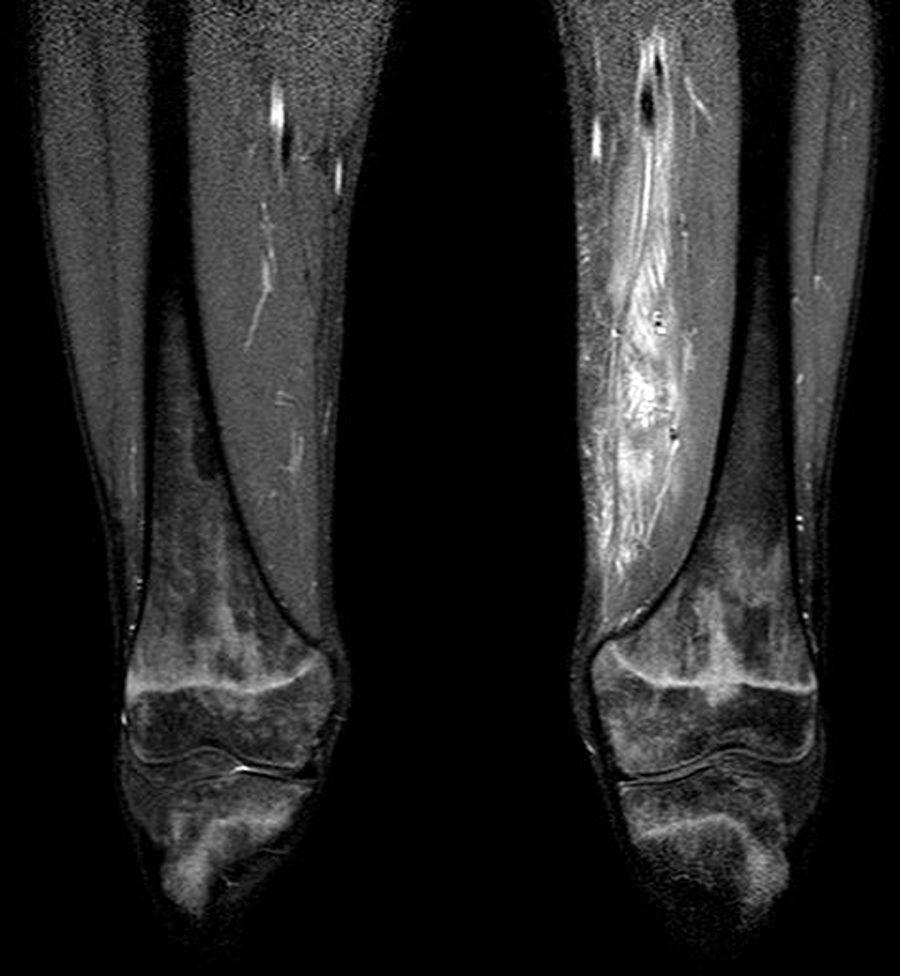
After three days of treatment, the patient persisted with the same symptoms showing no improvement. A soft tissue ultrasound reveled a dysfunctional muscle area in relation with the vastus medialis of quadriceps and the adductors muscles compatible with pyomyositis (Fig. 1). A MRI study confirmed the diagnosis (Fig. 2). Consequently, our department was consulted in order to consider surgical debridement. Finally he was taken to surgery performing a complete debridement and drainage of the muscle injury. Samples were collected and sent for microbiological study, identifying an infection due to E. coli as the causative agent.
After i.v. antibiotic treatment for 3 weeks and surgical debridement, the patient recovered satisfactorily and there were no problems in the healing process or post-surgical infections around the surgical wound. Leucocytes rose to 600×109/l and C-reactive protein descended until 140mg/dL. Nowadays, the episode of pyomyositis is totally resolved.
DiscussionUp to the date, only 20 cases of E. coli pyomyositis have been reported, most of them involving patients with different causes of immunodeficiencies such us AIDS and other hematologic malignancies related or not with previous chemotherapy.5–16 However, this one is only the second patient with idiopathic severe aplastic anemia reported presenting pyomyositis due to E. coli.
When pyomyositis occurs in immunocompromised patients, as in the case reported here, we may have doubts about the convenience of surgical debridement because of fear of well known complications described in this type of patients such are postoperative local infections or healing problems around the surgical wound.17–19 However, an early diagnosis, surgical debridement with complete drainage of the purulent material, together with antibiotic therapy, eradicates the infection in most patients.20,21
Although an initial antibiotic therapy for pyomyositis should include a broad-spectrum agent with good S. aureus coverage (can be modified based on antibiogram), coverage of gram-negative as E. coli, is advised to be empirically included in the treatment of immunocompromised patients.2
We report a further case of pyomyositis due to E. coli in an immunocompromised patient, only the second one associated to severe idiopathic aplastic anemia.
ConclusionsPyomyositis caused by E. coli is uncommon condition, and very few cases have been reported, most of them being severe immunodeficiency patients, but we should know the existence of this entity and its management. Although the pyomyositis is rare in our country, should be included in the differential diagnosis of patients presenting with fever, muscle pain and loss of function, especially in relation to chronic debilitating diseases and in subjects performing intense muscular exercise.22 Despite being a rare cause, we must include gram negative antibiotic for empirical therapy and surgical treatment, whenever possible, regardless of the fear of possible postoperative problems (infection and/or wound healing) when dealing with immunocompromised patients.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study have received sufficient information and have given their informed consent in writing to participate in that study.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence is in possession of this document.
Conflict of interestThe authors declare no conflict of interest.


